



Most prior research on resilience to HIV/AIDS has utilized quantitative tools (e.g., scales and surveys) to examine individual-level assets (e.g., self-efficacy, hope, optimism) that researchers believe represent or approximate resilience to HIV/AIDS with minimal consideration for the perspectives of men who have sex with men (MSM), the population that has remained at greatest risk of, and the most impacted by HIV/AIDS in North America since the 1980s. The aim of this qualitative study is to identify community-level resources that bolster resilience to HIV/AIDS based specifically on the perspectives and lived experiences of middle-aged and older (MAO) MSM living with HIV/AIDS. Employing a Community-Based Participatory Research (CBPR) approach involving the meaningful and active engagement of MSM at multiple levels (i.e., as research team members, peer researchers, Community Advisory Board representatives, community partners, and study participants), forty-one MAO MSM living with HIV/AIDS from Ontario, Canada, were included in the study’s semi-structured interviews. Utilizing thematic analysis, four major themes were identified from the interview data: (a) the 2SLGBTQ+ community; (b) community-based not-for-profit organizations; (c) public health services; and (d) neighbourhood support programs. This article discusses the value of community-level resources as important additions to individual-level assets for bolstering resilience to HIV/AIDS, as well as the implications of the study’s findings and limitations for future HIV/AIDS services and research.
Please click here to access the PDF version of this article, including tables and figures.
Since the beginning of the HIV/AIDS epidemic in the early 1980s, gay, bisexual, two-spirit, and other men who have sex with men (MSM) have remained the population most affected by HIV/AIDS in Canada (Haddad et al., 2019; Public Health Agency of Canada [PHAC], 2013) and the United States (Rhodes & Wong, 2016; Singh et al., 2018), and thus continue to be a crucial focus of population health and social science research today. Most extant research on HIV/AIDS among MSM has focused on MSM’s increased risk of, and vulnerabilities to HIV infection; leading many researchers to call attention to the limitations of deficits-based research (Halkitis et al., 2017; McNair et al., 2018). For example, in their article discussing prevention research for gay and bisexual men, Herrick and colleagues (2014) argued that interventions developed from strengths-based approaches may account for variances in health outcomes not identified in deficits-based research, and may very well increase participation of, and reach to, individuals who are most at risk. They pointed out that a resilience-focused approach to health disparities research among MSM could contribute to improving intervention effect sizes, and promoting health further through the identification of new variables and mechanisms for health promotion that can be incorporated into HIV/AIDS interventions (Herrick et al., 2014). In addition, Herrick and colleagues (2011) described resilience to HIV/AIDS among MSM as an “untapped resource” for behavioral intervention. They emphasized that harnessing naturally occurring strengths and resiliencies may further enhance already effective programs, which could provide additional effectiveness in reversing HIV transmission trends among MSM.
On the basis of a scoping review of strengths-based approaches to two-spirit, lesbian, gay, bisexual, trans, and queer (2SLGBTQ+) health research, Colpitts and Gahagan (2016) found the concept of resilience to be a key conceptual framework for understanding and measuring 2SLGBTQ+ health. Like Herrick and colleagues (2014), Colpitts and Gahagan (2016) championed the utility of resilience in health disparities research, particularly on different sexual and gender minority health foci (e.g., HIV/AIDS, depression, problematic substance use).
Resilience can be understood as “the element of risk being mitigated by protective factors to produce a positive outcome adjustment” (Stewart et al., 1999). It commonly refers to the ability to recover from, withstand, or overcome significant illness, stress, or adversity (Colpitts & Gahagan, 2016). Resilience has also been described as a “positive adaptation within the context of significant adversity” (Luthar et al., 2000), and theorized by scholars both as “a trait and a process” (Halkitis et al., 2017). In the context of living with HIV/AIDS, and for the distinct purpose of this article, resilience is defined and understood as the capacity to: (a) survive the clinical and social impacts of HIV/AIDS; (b) live full lives despite a chronic illness; (c) thrive despite challenges brought about by HIV stigma and discrimination; and (d) purposefully contribute to the goal of ending the HIV/AIDS epidemic.
Evidence for resilience among MSM is widespread in both scientific literature and historical accounts of sexual and gender minority culture (Colpitts & Gahagan, 2016; Herrick et al., 2014; Herrick et al., 2011). It is well documented that experiences of adversity such as 2SLGBTQ+ discrimination, and marginalization due to HIV stigma, are associated with increases in co-occurring psychosocial health problems (i.e., syndemics) that affect each other adversely and synergistically (Herrick et al., 2014; O’Leary et al., 2014). Despite this, research has shown that many MSM exhibit resilience to both the effects of adversity, and the impacts of HIV syndemics (Herrick et al., 2011), which has prompted researchers to study potential resilience factors (e.g., optimism, education) that may buffer against syndemics typically associated with higher rates of self-reported high-risk sexual behaviors and HIV infections (Hart et al., 2010; O’Leary et al., 2014; Stall et al., 2003).
Resilience can be expressed at individual-, collective-, or community-levels (Dulin et al., 2018; Emlet et al., 2010; Emlet et al., 2019; Torres de Carvalho et al., 2007). It has been described as a concept that is comprised of both individual-level assets (i.e., referring to internally held factors such as self-efficacy or coping skills), and collective- or community-level resources (i.e., factors external to the individual, such as parental support or community-based organizations), which enable individuals to withstand or overcome challenges in their lives (Dulin et al., 2018; Fergus & Zimmerman, 2005). While there has been some published research examining primarily individual-level (i.e., intrapersonal, interpersonal, and behavioral) intervention assets or attributes for promoting resilience to HIV/AIDS dedicated to the context of young MSM (Harper et al., 2014; Rhodes & Wong, 2016), there has been relatively little empirical research done to explore community-level resources for bolstering resilience to HIV/AIDS; particularly, research focused on middle-aged and older (MAO) [i.e., 40 years and older] MSM living with HIV/AIDS (PHAC, 2013), the subpopulation among all MSM living with HIV/AIDS that to this day continues to be most affected by HIV/AIDS since the start of the epidemic (Centers for Disease Control and Prevention [CDC], 2016; CDC, 2019; Haddad et al., 2019; PHAC, 2013).
Some researchers and community advocates have emphasized the importance of keeping in mind the resilience that MAO MSM have exhibited most of their lives in the face of institutionalized homophobia and ageism, mistrust of medical and social service institutions, mental health issues, and/or HIV stigma and discrimination in the healthcare system, as well as the community-level resources MAO MSM access and capitalize on to bolster their resilience to the clinical and social impacts of HIV/AIDS (Brotman et al., 2003; Emlet et al., 2010; Emlet et al., 2019; Genke, 2004; Halkitis et al., 2017). Related to this, the majority of research conducted on resilience to HIV/AIDS in the past decade has historically been quantitative studies that employed surveys, scales, and general measures to approximate the concept of resilience to HIV/AIDS, which were neither tailored for the context, nor developed with the perspectives and input, of people living with HIV/AIDS (PLWH) (Dulin et al., 2018; Gottert et al., 2019). The aim of the qualitative study discussed in this article was to address these apparent research gaps – in partnership with MAO MSM, identify and examine community-level resources that bolster resilience to HIV/AIDS based specifically on the perspectives and lived experiences of a diverse group of MAO MSM living with HIV/AIDS.
Method
For this qualitative study, a Community-Based Participatory Research (CBPR) approach (Israel et al., 1998) that emphasized the importance of community engagement, stakeholder partnership, and the greater and meaningful involvement of PLWH in population health research (Roy & Cain, 2001; Travers et al., 2008), was utilized. From the beginning of the research process, a collaborative relationship was established between the research team and the project’s primary community partner organization, Realize(https://www.realizecanada.org/en/). Realize is a community-based organization that fosters positive change for PLWH and other episodic disabilities. With the support of Realize, a Community Advisory Board (CAB), comprised of MAO MSM and providers from 2SLGBTQ+ agencies and AIDS service organizations (ASOs), was created to collaborate with the research team and community partners in order to identify and determine the study’s aim, methodology, and target population. The study’s aim, procedures, and intended conduct were reviewed and approved by the Research Ethics Board (REB) of the Centre for Addiction and Mental Health in Toronto, Canada.
Peer Researchers
MAO MSM were meaningfully involved in the project in several ways. MAO MSM were involved as research team and CAB members with the opportunity, agency, and autonomy to provide feedback and input at every stage of the research process. They were also involved as community-based organization partners supporting the study’s participant recruitment process; as study participants; and as peer researchers. In the context of the project, peer researchers were members of the research team from the community with lived experiences relevant to the study’s research questions. Two peer researchers were screened, selected, and provided training and financial compensation while they actively participated in the recruitment, scheduling, and co-interviewing of study participants, as well as in the project’s data management, analysis, and knowledge mobilization stages. Capacity-building aspects in the data collection, analysis, and dissemination stages of the project were adapted from an existing published modular curriculum (Eaton, 2019; Eaton et al., 2018; Ibañez-Carrasco et al., 2020). The research team and CAB members believed that these capacity-building aspects were very important to not only promote the meaningful and greater involvement of MAO MSM at risk of or living with HIV/AIDS in the project, but also increase opportunities to enrich all stages of the research process by incorporating the input of relevant stakeholders whose significant lived and work experiences were critical to achieving the study’s research aim and goals (Ibañez-Carrasco et al., 2019).
Participants
Study participants were recruited in accordance with recommendations from the CAB members and different community partners. Individuals were included in the study if they identified as MSM, were 40 years of age or older, and already living with HIV/AIDS for at least one year. They also had to reside in Central or Southwestern Ontario, Canada, at the time of the interviews. Prospective participants were invited to join the study using REB pre-approved ad flyers posted on the websites and at the premises of different 2SLGBTQ+ agencies and ASOs across Ontario, and REB pre-approved email recruitment messages sent out through participating community partners’ listservs. Forty-one MAO MSM living with HIV/AIDS participated in the study between February to June 2019. The participants represented a diverse group of MAO MSM living with HIV/AIDs in terms of age range, race or ethnicity, geographical area of residence, and other sociodemographic characteristics (Table 1).
Table 1. Participant Characteristics (N = 41)
Procedures
Participants were co-interviewed by the first author and one of the two peer researchers in 1-1.5 hour long, digitally recorded sessions, either at the office of one of the two interviewers, or in a secure room of a community-based organization of the participant’s choosing. Interviews followed a semi-structured interview guide, which was developed and finalized in collaboration with the CAB members and community partners. The guide utilized primarily open-ended questions to: (a) explore the lived experiences of the participants as MAO MSM living with HIV/AIDS; (b) identify community-level resources that participants believed bolstered their resilience to the clinical and social impacts of HIV/AIDS; and (c) examine the reasons why participants believed these community-level resources bolstered their resilience to HIV/AIDS.
Participants were sampled across Central and Southwestern Ontario until data saturation for major themes was reached (i.e., no new information relevant to the major themes emerged as additional interviews were conducted). Each participant provided informed consent prior to their interviews and received $25 as compensation for their time and participation. Interviews were transcribed verbatim by the peer researchers, and the transcripts were then verified by the first author prior to the data analysis.
Analysis
Due to its inherent flexibility, thematic analysis (Braun & Clarke, 2006) was chosen as the method to analyze the interview data. It was deemed the best approach to fulfill the study’s aim because its epistemological and theoretical freedom allowed for a flexible examination of the different perspectives derived from the diverse interview sources.
Because of the significant likelihood that the project’s other research team members, CAB members, and community partners would personally know many of the prospective MAO MSM living with HIV/AIDS who would participate in the interviews from their previous work interactions, the raw data were only made accessible to the interviewers (i.e., the first author and peer researchers). This decision was made to allay prospective participants’ reluctance and apprehensions on the possibility of being identified in the interview transcripts and further ensure privacy and confidentiality in the research process.
The first author and the two peer researchers conducted the initial phase of the analysis. Prior to coding, the first author read and re-read all the interview transcripts to gain intimate knowledge of the data, and then chose 10 transcripts that would represent the data set in terms of participant characteristics, perspectives, and contexts (e.g., age range, race or ethnicity, geographical area of residence) for the two peer researchers to read and re-read. As separate coders, the first author and the two peer researchers identified initial codes, and then searched and reviewed for themes from the 10 representative transcripts. Next, the three coders met and compared their initial codes and themes. Together, they defined and named emerging codes, subthemes, and themes to create a codebook, which they used for the analysis of the remaining 31 transcripts. The three coders then independently employed selective coding on the remaining 31 transcripts using the codebook to refine the findings of the interview data in an iterative process. After this initial phase of the analysis, the three coders produced a de-identified report containing the themes, subthemes, and supporting quotes for the rest of the research team and CAB members to review. At subsequent phases, the rest of the research team and the CAB members reviewed the de-identified report with aggregated data, and provided feedback on the themes, subthemes, extracts, and overall quality of the report. This process was conducted using different techniques to establish credibility (i.e., source triangulation), confirmability (i.e., reflexivity, analyst triangulation), transferability (i.e. thick description), dependability (i.e. external audit), as well as uphold the trustworthiness and rigor of the study’s findings and analysis (Lincoln & Guba, 1985).
While several themes were identified from the interview data during the analytic process, this article focuses specifically on themes pertaining to the community-level resources that participants identified and believed bolstered their resilience to the clinical and social impacts of HIV/AIDS. Pseudonyms were used for each participant to maintain their anonymity and privacy.
Results
Four major themes related to community-level resources that bolster resilience to the clinical and social impacts of HIV/AIDS were identified based on the perspectives and lived experiences of the participants. The themes were: (a) the 2SLGBTQ+ community; (b) community-based not-for-profit organizations; (c) public health services; and (d) neighbourhood support programs. Although some of the community-level resources that the participants identified were sources of emotional and social support for them, the resources described in this article were included in this section because they were primarily discussed by the participants as resources that bolstered resilience to the clinical and social impacts of HIV/AIDS in other specific ways, in addition to being sources of emotional and social support.
The 2SLGBTQ+ Community
According to more than half of the participating MAO MSM living with HIV/AIDS, the presence of an established 2SLGBTQ+ community in Toronto and the other urban areas in Southwestern and Central Ontario at the time of their HIV/AIDS diagnosis was a huge resource for them in terms of overcoming the clinical and social impacts of HIV/AIDS. They revealed that from word-of-mouth spread of information in the 2SLGBTQ+ community, they were able to gather important facts on HIV; news on where to find family doctors, HIV specialists, and mental health professionals who could help them; and updates on clinical treatments and community services. The participants stated that aside from being a source of vital information, the 2SLGBTQ+ community was also a valuable resource in terms of different types of support during the early epidemic. Many MSM came together to assist and console each other; lesbian women stepped up to provide practical care; queer community members connected them to needed health and social services; and drag queens tirelessly raised funds. Gary recalled, “We all became increasingly aware of how amazing drag queens are at fund-raising for causes in our community.” The 2SLGBTQ+ community also became a primary resource for socialization and social support. Jonathan explained,
“I gradually started coming out and disclosing my [HIV] status to people in the community. That was helpful, it started taking the pressure off [me]. I could just be myself with more and more people. They were supportive. There were lots of other queer folks around, including role models I could look up to. I started building my social network, and eventually, the majority of my friends were from the queer community.”
Members of the 2SLGBTQ+ community gathered together in solidarity to look out for each other, organize human rights campaigns, and advocate for their most basic needs, especially for those who were recently diagnosed with HIV/AIDS. These actions led to the creation of different activist groups, grassroots movements, local agencies, and service organizations in Toronto, and eventually, across the province of Ontario; all of which were dedicated to address the dire circumstances of MSM living with HIV/AIDS at that time. The 2SLGBTQ+ community also gave the participants an opportunity to become productive despite their challenges and feel good about their productivity. Pat recalled his earlier experiences in Toronto,
“I participated and did a lot of non-profit work in the community. I believed that was part of my therapy in getting over the loss [of many people to HIV/AIDS]. Trying to give something back to the community. It was for my mental health. Because I had education as an aboriginal person that many others didn’t, I always felt it was important to give back. I wanted to make sure aboriginal issues were brought forward in the community.”
Community-Based Not-For-Profit Organizations
The second theme that was identified in the interview data as community-level resources bolstering resilience to HIV/AIDS based on the perspectives and live experiences of MAO MSM living with HIV/AIDS was community-based not-for-profit organizations. There were two types of community-based not-for-profit organizations that participants pointed out and discussed in the interviews: (a) 2SLBTQ+ agencies, and (b) ASOs. Even before they were diagnosed with HIV/AIDS, many participants were already accessing services related to HIV/AIDS (i.e., information, prevention programs, referrals) from both 2SLGBTQ+ agencies and ASOs.
2SLGBTQ+ Agencies
Nearly one fifth of participant specifically mentioned how helpful 2SLGBTQ+ not-for-profit agencies in the community were over the years. 2SLGBTQ+ not-for-profit agencies increasingly provided much needed services and referrals to them, especially in the last thirty years. The 519 (known then as the 519 Church Street Community Centre) and the Gay Men’s Sexual Health Alliance were repeatedly mentioned in a positive light by participants. Among the services and programs these agencies provided, assistance with referrals to doctors and other healthcare and support services, information about HIV prevention, venues for stakeholder gatherings and meetings, and refugee and legal aid services, were the most singled out in the interviews. Arthur described his earliest experiences with using The 519 as a resource:
"When I first arrived in Canada from [country of origin], I got in touch with The 519. They hooked me up with legal aid, welfare, and where I could get medical attention. They gave me a bunch of references for places to go to get help. That meant a lot. They had programs for refugees to help newcomers with the process. There were meetings, and you were supposed to get a stamp, and that was supposed to prove that you were gay. Eventually, The 519 was also a place I could go to meet people, get fed, and later, volunteer to keep busy."
AIDS Service Organizations
The most appreciated type of community-level resource that over 60% of the participants identified was ASOs. Whether participants were from Downtown Toronto, the Greater Toronto Area, or in other areas of Southwestern Ontario, many of them had a strong appreciation for the different services and programs that ASOs provided. Many of the participants accessed services and programs from two or more ASOs. Often, participants mentioned that availing of services in one of the ASOs led to services at other ASOs and agencies that provided help they needed to survive and thrive while they were trying to overcome the challenges of living with HIV/AIDS. The support groups and drop-in services of the different ASOs, in particular, were important resources for overcoming isolation and feelings of helplessness, which many participants experienced at different times over the years.
Over half of the participants from the study shared that at one point or another in their life, they accessed services from the AIDS Committee of Toronto (ACT), which they believed were very useful, if not essential (ACT continues to be one of the largest ASOs in Central and Southwestern Ontario). For several years, ACT practically the only existing ASO they could turn to after learning of their HIV/AIDS diagnosis. The services at ACT that they availed of the most included counselling, group programming, community health forums and workshops, financial assistance, income tax clinics, lunch programs, and referrals to other healthcare and social service providers. Ricky recounted the different services at ACT that he and his friends used for many years,
“ACT’s buddy program connected me with this guy that helped me get care in my home. We actually became friends as I became healthier throughout my whole ordeal. Through the years, ACT has had all sorts of group programming my friends and I would join…Many years later, I needed counselling and got that from ACT too. They also referred me to a Rainbow [counselling] program at the Centre for Addiction and Mental Health…One thing that ACT actually specializes in is education. They always have different workshops and forums, if you’re interested in learning about new things.”
Half of the study participants also availed of services from the Toronto People with AIDS Foundation (PWA). Many of these participants expressed appreciation for the more practical supports PWA provided, such as the food bank, assistance with applications to the Ontario Disability Support Program (ODSP), community engagement programs, and access to therapeutic programs like massage therapy, physiotherapy, and acupuncture. Jeremiah appreciated PWA’s practical programming, “I went to PWA for the first-time last year for information I needed about the ODSP application. They guided me through all steps. It’s a very good organization!”
Nearly a third of study participants living with HIV/AIDS mentioned how Casey House (formerly an AIDS hospice and now a specialty hospital for PLWH) had either saved their life or provided them a new lease in life. Jack shared in his interview, “I lived at Casey House for eight months. They took care of me. They literally saved my life!” Many participants stayed at Casey House for some time primarily for convalescence, especially in their earlier years of struggling with the clinical impacts of HIV/AIDS, and several of them availed of wellness services at Casey House such as yoga and meditation.
Many participants identified different types of resources from other ASOs that they also found helpful during their years of struggle, including: (a) research, information, and advocacy from the Canadian AIDS Treatment Information Exchange, the Ontario HIV Treatment Network and the Ontario AIDS Network; (b) housing support from Fife House; and (c) legal aid and support from the HIV/AIDS Legal Clinic Ontario and Prisoners with HIV/AIDS Support Action Network. Racial minority, immigrant, and newcomer participants, in particular, specifically commended ethno-specific ASOs for their work over the years, and these ASOs included the Alliance for South Asian AIDS Prevention, Asian Community AIDS Services (ACAS), Black Coalition for AIDS Prevention, Centre for Spanish-Speaking Peoples, and Latinos Positivos. Juan expressed his gratitude for the help he received when he first came to Canada, “Although they don’t have as much resources as the bigger ASOs, Latinos Positivos is really good for newcomers with language barriers and don’t speak English much.” Jin also had similar praise for another ethno-specific ASO, “It’s great to go to ACAS. They have case workers who look like me and have the same or similar culture and language as mine. It makes it much easier to get help from them.”
Finally, the ASOs that were repeatedly mentioned by participants who lived outside of Downtown Toronto in appreciation of these ASOs’ diverse services and programs included the AIDS Committee of Cambridge, Kitchener, Waterloo, and Area; AIDS Committee of Durham Region; AIDS Committee of York Region [now CAYR Community Connections]; HIV/AIDS Resources and Community Health Guelph; Peel HIV/AIDS Network [now Moyo Health and Community Services]; Regional HIV/AIDS Connection London; and The AIDS Network of Hamilton, Halton, Haldimand, Norfolk, and Brant.
Public Health Services
Public health services were the third theme that was identified in the thematic analysis of the study’s interview data. Under public health services, two sub-themes emerged: (a) community health clinics and centres, and (b) excellent healthcare and service providers. These two sub-themes are discussed in the next sub-sections.
Community Health Clinics and Centres
Approximately 40% of the MAO MSM living with HIV/AIDS who took part in the interviews shared with us how vital it was to their survival, health, and wellbeing to have access to community health clinics and centres. Many participants mentioned that the Hassle-Free clinic in Toronto was instrumental not only in providing the confidentiality they needed upon learning of their HIV/AIDS diagnosis, but also with getting through the earliest stages of their acceptance and adjustment to living with HIV. Hassle-Free clinic was an important resource not only in terms of ensuring confidential HIV testing, but also gaining counselling and information about HIV, doctors, specialists, and related services. Donald narrated his first visit to Hassle-Free clinic and how his long-standing relationship with it began,
“I was constantly working back then, feeling tired and fatigued, and getting colds. Getting rid of one cold, then getting another one. Yet, I couldn’t take time off work. That went on for almost a couple of years. Then I thought, I should just get checked out. I learned about the clinic and anonymous testing from a flyer. I went to Hassle-Free, and that’s how I found out [about my HIV]. Hassle-Free gave me a booklet with a list of doctors. That’s how I got my family doctor. I see my doctor regularly, and I also go to Hassle-Free clinic if I think that something is not going well. I go to Hassle-Free clinic to get my test results. I also volunteer over there. I started volunteering because it was just easier to get my testing because l was there.”
Numerous participants also attributed the initiation and continuity of their HIV care to other community health clinics and centres such as Sherbourne Health, and the Regent Park, Parkdale Queen West, and High Park community health centres. Glenn described how his healthcare became more consistent because of his access to a community health centre,
“I’ve been tied to a community health center for a while now, the one at Regent Park. They have a nurse practitioner, and my HIV doctor. I don’t know when he became my regular doctor. But they kept assigning me the same doctor. Eventually, he took my case. I have my family doctor for general things and my TB at Regent Park too.”
Excellent Healthcare and Service Providers
A third of the respondents profoundly and specifically expressed gratitude for the excellent care they received from the different healthcare and service providers over the years. On the top of their list of providers to thank are their family doctors. Family doctors who were knowledgeable, caring, non-judgmental, and gay/bi-positive received the most praise. Some participants said they had physicians who not only provided great health services, but also emotional support. Francis praised his family physician, “My doctor’s the best! He’s very knowledgeable, goes out of his way to explain things to me, and he builds me up…” Additionally, several respondents mentioned that it was a huge relief to have openly gay family doctors either because they had a better understanding of them and their coping strategies as patients, or because they did not have to explain or even guide their doctors in terms of what they specifically needed or wanted as MSM living with HIV/AIDS. Joseph talked about how he found his family doctor and stayed with him ever since:
“I guess I was a little bit ahead of the curve back then. I sought out and found a gay doctor…he was the only resource [about HIV] that I had at that time. He’s the one who did the blood test. That’s when I found out about the HIV and he prescribed me my medications. Back then, you had to decide to get tested on your own, no one would test for it unless you had a gay doctor. I’ve stayed with him ever since.”
HIV physician specialists were also highly endorsed by participants as vital providers who gave them very specialized care. HIV specialists who were up-to-date on the newest HIV medications and treatments were most appreciated by participants who experienced AIDS complications at some point in their life, and who had nearly succumbed to their life-threatening conditions. A close second mention were psychiatrists/counsellors (from places such as St. Michael’s Hospital, David Kelley 2SLGBTQ+ and HIV/AIDS Counselling Services, and Mt. Sinai Hospital) who supported and promoted participants’ mental health, particularly when they experienced isolation, depression, and suicidal ideation. Bryan described how counselling helped change his life,
“When I tested positive, I would go to the clinic once a week for counselling. It was a very good program. She was an excellent counsellor. It was the kind of counselling I should have had when I was getting divorced. Talking about my kids and my ex. I was comfortable. I could be honest and open, and nobody would blink an eye. I was just like everybody else. That’s why I say HIV was almost like a blessing because it opened up the doors to a lot of things in my personal life that I couldn’t talk about or do before.”
A recurring comment was how much gratitude respondents had for kind and competent social and case workers who helped them pick up their lives by assisting them with ODSP applications, transitional housing, job searches and applications, food security, referrals to healthcare and social services, and much needed socialization. Psychiatrists, counsellors, and social and case workers were able to help the participants get through the darkest days of their lives. Denis expressed his appreciation for the assistance he received from his case worker, “I had no support from my family. My case worker and therapist were my only support. They got me stabilized with housing. That was a huge step.”
Neighbourhood Support Programs
The fourth and final theme that was identified in the analysis of participant interviews was neighbourhood support programs, which included (a) homeless shelters and transitional housing, and (b) harm reduction and needle exchange programs, as community-level resources for bolstering resilience to the clinical and social impacts of HIV/AIDS.
Homeless Shelters and Transitional Housing
As MAO MSM living with HIV/AIDS, some of the participants found themselves in need of financial assistance and with very little opportunities to earn a decent wage after their HIV/AIDS diagnosis. Some were let go from their jobs after incidents of inappropriate disclosure of their HIV status by others, some became too sick to sustain employment, and others lost the support of their families when they voluntarily disclosed their HIV status.
Participants shared stories about how homeless shelters and transitional/supportive housing such as Seaton House, Fife House, John Gordon Home, Leap of Faith Together Community Services and McEwan Housing and Support Services, Fred Victor, and Salvation Army provided them with shelter, housing, food, and other services when they were homeless, hungry, and could not catch a break after contracting HIV. For many of them, as MSM struggling with the impacts of living with HIV/AIDS, these establishments helped them survive and get back on their feet. Abraham described his experiences of being homeless, recovering from the complications of HIV/AIDS, and then having no place to live immediately after his recovery:
"It was eight years ago. It was hard as hell [being homeless]. You’re on your own. No one cares. No one bothers to say, “You need a helping hand?” Nothing. A lot of homeless stuck together. We were like a family. We looked out for each other. I had to access a shelter. The first shelter I went to was a shelter for homeless people, and also people who were struggling with mental health issues. It was very difficult because I've never been in such a situation before. I later went to Salvation Army, and then to Seaton House. At some point, I got really sick, and when I came out of the hospital, I had no place to go after recovering from a coma. Eventually, Fife house helped me with an apartment. Without the housing support and the shelters, I wouldn’t have known where I would be."
Harm Reduction and Needle Exchange Programs
Although most did not go into detail about it, several participants felt that it was worth mentioning how important it was for their survival and recovery to have had access to harm reduction and needle exchange programs in the community, especially when they needed to get through their roughest moments. The participants expressed that these programs allowed them to overcome issues related to their substance use without fear of judgment or consequences. Alex explained:
"I’m all for these programs. I was addicted for three years…maybe even five years. I used a couple of them. Like The Works…on Victoria and Dundas. When I was on the street, I used them a lot. They were pretty much easy to access. A lot of the girls and guys that work the streets, they know. We got free supplies when we were injecting meth. I had no idea I could get stuff I was paying for in Shoppers Drug mart for free. It never occurred to me. I am a pragmatist. If something works, and it reduces harm to a person, or limits the harm to them and the rest of the community…then it’s probably good. The needle exchange programs, they help prevent the spread of disease. I have HIV, but I can still get Hepatitis B and C."
Discussion
This is the first CBPR qualitative study to identify and examine community-level resources that bolster resilience to the clinical and social impacts of HIV/AIDS from the direct input, perspectives, and lived experiences of MAO MSM living with HIV/AIDS; the population that has been most affected by HIV/AIDS since the start of the epidemic in North America (Haddad et al., 2019; PHAC, 2013; Rhodes & Wong, 2016; Singh et al., 2018). During the analysis of the study’s interview data, four major themes were identified as community-level resources that bolster resilience to HIV/AIDS: (a) the 2SLGBTQ+ community; (b) community-based not-for-profit organizations; (c) public health services; and (d) neighbourhood support programs. Although these different community-level resources may have been discussed in prior academic literature as factors that are relevant to the health and wellbeing of MSM, this is the first time that MAO MSM living with HIV/AIDS have categorically and collectively classified them in an empirical study as resources that have bolstered their resilience to HIV/AIDS based on their personal perspectives and lived experiences. The rich descriptions and stories they shared serve as testimony to the value of these community-level resources in bolstering resilience to HIV/AIDS. Because this study has directly verified and confirmed from MAO MSM living with HIV/AIDS themselves the significant value of these community-level resources as extraneous factors that bolster their resilience to HIV/AIDS, it is reasonable to propose that these community-level resources are important factors to consider in HIV care, programs, services, and policies, not only as resources that could be utilized to support MAO MSM living with HIV/AIDS in general, but more importantly from the standpoint of promoting health equity and addressing health disparities, be used to equitably support MAO MSM living with HIV/AIDS who may not possess inherent qualities or have as much access to individual-level assets for building resilience to HIV/AIDS compared to other people and MAO MSM living with HIV/AIDS. Community-level resources for bolstering resilience to HIV/AIDS could serve as important factors for promoting equity even among MAO MSM living with HIV/AIDS themselves, who may not necessarily experience the same challenges and have access to the same individual-level resources.
Valuing Resilience to HIV/AIDS in Community Psychology Practice to Promote Equity among MAO MSM living with HIV/AIDS
Prior to this article, the vast majority of peer-reviewed articles on resilience to HIV/AIDS has not explicitly defined ‘resilience’ in their discussions (Gottert et al., 2019). For publications on HIV resilience research that have provided their definition of ‘resilience’, most described resilience only at the individual-level (e.g., psychological); with few including limited interpersonal-level resilience (e.g., social support). For a long period of time, there had been a predominance of quantitative studies using general measures of resilience to HIV/AIDS (mostly as assets related to individual personality characteristics), which were not tailored to the contexts and needs of PLWH as a community (Dulin et al., 2018; Gottert et al., 2019). Scales and surveys on self-efficacy, hope, optimism, coping strategies, quality of life, stress, depression, and social support (Dulin et al., 2018; Earnshaw et al., 2015; Emlet et al., 2013; Emlet et al., 2017; Fang et al., 2015; Gottert et al., 2019; Logie et al., 2014; Sinclair & Walston, 2004; Spies & Seedat, 2014; Thurston et al., 2018), have been used by many researchers outside of Community Psychology to examine and circumlocutorily discuss resilience to HIV/AIDS, without directly taking into consideration the perspectives and lived experiences of MSM living with HIV/AIDS from the community, especially MAO MSM living with HIV/AIDS, many of whom have remained resilient to HIV/AIDS the longest. Although there are a few exceptions to this trend (Emlet et al., 2010; Gigliello & Ackerman, 2019; Harper et al., 2014), most prior studies have, at best, discussed resilience to HIV/AIDS based on measures of factors that researchers believed represented resilience of people to the clinical and social impacts of HIV/AIDS. Despite the fact that most of these measures have been proven to have good psychometric properties (Gottert et al., 2019), they also have a significant limitation that is very difficult to ignore. These measures have been used to examine factors that approximate resilience to HIV/AIDS; factors that have not necessarily been ratified or affirmed by the perspectives and lived experiences of the most relevant community stakeholders.
At the core of the practice of Community Psychology is the imperative to value and utilize what is most useful and important to the relevant community stakeholders of the critical research focus being investigated. In terms of resilience to HIV/AIDS as a focus, many early conceptualizations have depicted it as a static, stable construct with limited attention paid to social context and broader systems that may bolster or hinder resilience across time and place (Harrison & Li, 2018). Fortunately, more recent research studies on resilience to HIV/AIDS have begun to discuss the concept of ‘resilience’ beyond protective factors in terms of individual assets, personal characteristics, and social support (Torres de Carvalho et al., 2007), and have specifically incorporated in their discourse the merits of community engagement, participation, empowerment, and most relevant to the study discussed in this article, resources at the community-level (Brennan et al., 2013; Dulin et al., 2018; Earnshaw et al., 2015; Ebersohn & Ferreira, 2011; Emlet et al., 2010; Emlet et al., 2019; Gottert et al., 2019; Kurtz et al., 2012; Solomon et al., 2019). The interview participants of the study featured in this article have explicitly identified and described the 2SLGBTQ+ community, 2SLGBTQ+ not-for-profit agencies, ASOs, community health clinics and centres, excellent healthcare and service providers, homeless shelters and transitional housing, and harm reduction and needle exchange programs as vital community-level resources that have bolstered their resilience to the clinical and social impacts of HIV/AIDS over the years. Hence, it is imperative for community psychologists to seriously consider and value these community-level resources in their practice, not only to help bolster the resilience of MAO MSM to HIV/AIDS, but also as factors that could potentially promote equity among all of them.
Community-level Resources that Bolster Resilience to HIV/AIDS: Implications for Community Psychology Practice
Although not always necessarily from the specific viewpoint of a resilience framework, published academic literature has, in fact, extensively discussed the various community-level resources that have been identified and described in this article in relation to HIV/AIDS. Together with existing literature on HIV/AIDS research, the findings and lessons learned from this study have specific implications for the practice of community psychologists whose work focuses on promoting the resilience and wellbeing of MSM living with HIV/AIDS.
The 2SLGBTQ+ community
In different studies, the 2SLGBTQ+ community has been described as a networked community that in the last few decades has become a source of MSM leadership, empowerment, and advocacy, especially for health promotion and services, and HIV research (Gigliello & Ackerman, 2019; Landers et al., 2011; McConnell et al., 2018; Trapence et al., 2012). Studies have found that access to the 2SLGBTQ+ community meant greater access to much needed resources for MSM (Meyer, 2015). Research has shown the mediating role of an individual’s connection to the 2SLGBTQ+ community to both tangible and intangible resources against minority stress (McConnell et al., 2018). The 2SLGBTQ+ community has been documented as a productive setting for overcoming adversity and building capacity and strengths (Gigliello & Ackerman, 2019); initiating campaigns and organizing activities for reducing sexual health risks and promoting HIV prevention programs (Landers et al., 2011); and generating novel ideas for transformative change (Meyer, 2015). Perhaps more than other researchers and scholars from other Psychology sub-disciplines, community psychologists would be able to appreciate and support the intrinsic worth of promoting what the 2SLGBTQ+ community could offer to MSM living with HIV/AIDS in their research and practice.
Community-based not-for-profit organizations
Within 2SLGBTQ+ communities, access to civil society and community-based not-for-profit organizations such as 2SLGBTQ+ agencies and ASOs have led to greater awareness of issues relevant to the larger community among MSM (James, 2005); opportunities for community involvement (Paceley et al., 2015); and avenues for developing self-esteem and social support networks (Paceley et al., 2016). From the time they were first established in the early 1980s (Poindexter, 2007), ASOs have been documented to be the most accessible resource in the community for dependable information and education on HIV/AIDS (Huber & Machin, 1995; Kwait et al., 2001). ASOs have also become reliable hubs for acquiring information on, and referrals to, important services that MSM at risk of or living with HIV/AIDS need (Kwait et al., 2001); volunteering and promoting activism in support of increased funding for research on HIV/AIDS issues (Flicker et al., 2009); and advocating for the greater and meaningful involvement of PLWH in the development and implementation of research, services, programs, and policies that would impact their health and wellbeing (Paterson et al., 2014; Travers et al., 2008). Based on the findings of this study, community psychologists could advocate for the establishment of more 2SLGBTQ+ agencies and ASOs in locations that need them the most, such as densely populated cities, rural and remote regions, and other underserved areas; conduct research on the potential benefits of creating different types of ASOs (i.e., large mainstream, service-specific, and ethno-specific or racial/ethnic minority-serving) in communities; and promote programs within existing 2sLGBTQ+ agencies and ASOs that the participants highlighted in their interviews as the most helpful and beneficial to them.
Public health services
Academic literature has long underscored the important role of public health services in supporting the health and wellbeing of aging MSM. Research has documented the significant value of community health clinics and centres in establishing the early diagnosis of sexually transmitted infections (STIs), especially HIV, among MSM (Mayer et al., 2009). More importantly, research has shown that community health clinics and centres have been key to the promotion of greater accessibility to sexual health services (e.g., the provision of condoms, lubricants, and STIs testing) and information (Arreola et al., 2015); the asymptomatic screening of STIs and the initiation of the continuum of HIV/AIDS care (e.g., diagnosis and referrals to treatment) among MSM (Hoover et al., 2010); and even the sustained engagement of MSM in the healthcare system prior to an HIV/AIDS diagnosis, and its crucial link to subsequent positive HIV/AIDS care outcomes (Axelrad et al., 2013). Research has also shown the critical part that healthcare and service providers play in the provision of culturally competent HIV/AIDS care, particularly with the adoption of MSM-affirming non-verbal communication; expression of respectful responses to HIV disclosures; and use of accepting and inclusive language in the healthcare and social service systems (Brooks et al., 2018; Quinn et al., 2015; Rossman et al., 2017; Rounds et al., 2014). Particularly in light of the testimonies of the study participants, community psychologists could play a vital role in maximizing that critical connection between the importance of public health services in bolstering resilience to HIV/AIDS and supporting MSM living with HIV/AIDS, who may not necessarily have the needed individual-level assets to thrive.
Neighbourhood support programs
Finally, scholarly publications have showcased the benefits of MSM accessing neighbourhood support programs such as homeless shelters and transitional housing, as well as harm reduction and needle exchange programs. Housing has long been considered a structural intervention with a substantial potential to reduce HIV risk and improve sexual health outcomes (Kidder, Wolitski, Royal, et al., 2007). With housing programs, people at risk of or living with HIV/AIDS are more likely to use condoms and have a fewer number of sexual partners (Marshall et al., 2009). Housing has also been documented as an important mechanism for improving the health of homeless PLWH, specifically in terms of supporting their medication adherence, and both their physical and mental health outcomes (Kidder, Wolitski, Campsmith et al., 2007). Notably, the feasibility and acceptability of modifying harm reduction strategies to the different contexts of MSM have already been empirically established (Rose et al. 2006), particularly in support of the efficacy and cost effectiveness of needle exchange programs (Carrico et al., 2014; Li et al., 2012). In their research and practice, community psychologists could purposefully highlight what may not be as immediately apparent to many users and providers of HIV services – that neighbourhood support programs such as homeless shelters, transitional housing, and harm reduction and needle exchange programs are integral to bolstering the resilience of many HIV-positive MSM to the adverse clinical and social impacts of HIV/AIDS.
Conclusion
This study adds important knowledge to current academic literature by identifying and determining specific community-level resources as valuable additions to the individual-level assets and interpersonal characteristics of MSM for building and bolstering resilience to HIV/AIDS, particularly from the perspectives of the community stakeholders that have exhibited resilience to HIV/AIDS the most since the beginning of the epidemic in North America. However, it is necessary to acknowledge the study’s limitations. It is important to note that the majority of participants who shared their personal accounts in the interviews were from Downtown Toronto, and that the community-level resources that were identified in the interviews were accessible mostly in Downtown Toronto and the other major urban cities of Central and Southwestern Ontario, Canada. The most significant implication of this limitation, therefore, is that these community-level resources will likely only be able to bolster resilience among MAO MSM living with HIV/AIDS if they have easy access to these resources found in Downtown Toronto and other major urban Ontario cities. This underscores the need for community psychologists to establish more advocacy and action for developing and establishing the identified community-level resources in more peri-urban, suburban, and rural areas to make such services more accessible to a greater number of MAO MSM living with HIV/AIDS. Related to this, as Canadians, it is important to note that the study participants have had access to publicly-funded healthcare and social services, which may not be the case for other MAO MSM living with HIV/AIDS who may be residing in locations without universal healthcare or health services.
Despite the large number and relative diversity of the study’s interview participants in terms of age range, race/ethnicity, and geographical location, the study has the same fundamental limitation that all qualitative studies have, which is that its data could not be statistically representative of the perspectives of all MAO MSM living with HIV/AIDS. For future studies on resilience of MAO MSM to HIV/AIDS, researchers could conduct quantitative studies that would complement the research aim and goals of this qualitative study. They could potentially use the study’s findings and analysis to develop and create new scales or measures that would examine the perspectives of MAO MSM on their resilience to HIV/AIDS and obtain results that would provide statistical significance and representation. Researchers may also consider conducting mixed methods approaches that would follow up and capitalize on the findings of the study. This study establishes a foundation for future research on resilience to HIV/AIDS that distinctly builds on the invaluable perspectives and lived experiences of MAO MSM living with HIV/AIDS.
Funding
This project received funding from the Canadian Institutes of Health Research Operating Grant – HIV/AIDS Community-Based Research Program (funding reference # 156917), as well as salary support from the Endgame Student Leader Award in HIV and Aging (EFP-1100) provided by the Ontario HIV Treatment Network. The authors of the article have no conflict of interests to declare.
References
Arreola, S., Santos, G.M., Beck, J., Sundararaj, M., Wilson, P.A., Hebert, P., Makofane, K., Do, T., & Ayala, G. (2015). Sexual stigma, criminalization, investment, and access to HIV services among men who have sex with men worldwide. AIDS and Behavior, 19, 227-234. DOI: 10.1007/s10461-014-0869-x.
Axelrad, J.E., Mimiaga, M.J., Grasso, C., & Mayer, K. (2013). Trends in the spectrum of engagement in HIV care and subsequent clinical outcomes among men who have sex with men (MSM) at a Boston community health center. AIDS Patient Care and STDs, 27(5). DOI: 10.1089/apc.2012.0471.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3, 77–101. DOI: 10.1191/1478088706qp063oa.
Brennan, D., Emlet, C., Brennenstuhl, S., Rueda, S., & the OHTN Cohort Study Research Team and Staff. (2013). Socio-demographic profile of older adults with HIV/AIDS: Gender and sexual orientation differences. Canadian Journal of Aging, 3(1), 31-43. DOI: 10.1017/S0714980813000068.
Brooks, H., Llewellyn, C.D., Nadarzynski, T., Pelloso, F.C., Guilherme, F.D.S., Pollard, A., & Jones, C.J. (2018). British Journal of General Practice. DOI: 10.3399/bjgp18X694841.
Brotman, S., Ryan, B., & Cormier, R. (2003). The health and social service needs of gay and lesbian elders and their families in Canada. Gerontologist, 43, 92-102.
Carrico, A.W., Flentje, A., Gruber, V.A., Woods, W.J., Discepola, M.V., Dilworth, S.E., Neilands, T.B., Jain, J., & Siever, M.D. (2014). Community-based harm reduction substance abuse treatment with methamphetamine-using men who have sex with men. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 91(3), 555-567. DOI: 10.1007/s11524-014-9870-y.
Centers for Disease Control and Prevention. (2016). People with diagnosed HIV in the US and dependent areas by age. http://www.cdc.gov/ hiv/library/reports/hiv-surveillance.html Accessed 05-03-2020.
Centers for Disease Control and Prevention. (2019). HIV Surveillance Report, 2018 (Preliminary); vol. 30. http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. Accessed 05-03-2020.
Colpitts, E., & Gahagan, J. (2016). The utility of resilience as a conceptual framework for understanding and measuring LGBTQ health. International Journal for Equity in Health, 15, 60-67. DOI: 10.1186/s12939-016-0349-1.
Dulin, A.J., Dale, S.K., Earnshaw, V.A., Fava, J.L., Mugavero, M.J., Napravnik, S., Hogan J.W., Carey, M.P., & Howe, C.J. (2018). Resilience and HIV: A review of the definition and study of resilience. AIDS Care, 30, 1–12. DOI: 10.1080/09540121.2018.1515470.
Earnshaw, V.A., Lang, S.M., Lippitt, M., Jin, H., & Chaudoir, SR. (2015). HIV stigma and physical health symptoms: do social support, adaptive coping, and/or identity centrality act as resilience resources? AIDS and Behavior, 19(1):41–9. DOI: 10.1007/s10461-014-0758-3.
Eaton, A.D. (2019). Filmed simulation to train peer researchers in Community-Based Participatory Research. Social Work Research, 43(3), 195–199. DOI: 10.1093/swr/svz011.
Eaton A.D., Ibañez-Carrasco, F., Craig, S., Carusone, S.C., Montess, M., Wells, G.A., & Ginocchio, G.F. (2018). A blended learning curriculum for training peer researchers to conduct community-based participatory research. Action Learning: Research and Practice, 15(2), 139-150. DOI: 10.1080/14767333.2018.1462143.
Ebersohn, L., & Ferreira, R. (2011). Coping in an HIV/AIDS-dominated context: Teachers promoting resilience in schools. Health Education Research, 26(4), 596-613. DOI: 10.1093/her/cyr016.
Emlet, C., Fredriksen-Goldsen, K., & Kim, H. (2013). Risk and protective factors associated with health-related quality of life among older gay and bisexual men living with HIV disease. Gerontologist, 53(6), 963-72. DOI: 10.1093/geront/gns191.
Emlet, C., Fredriksen-Goldsen, K., Kim, H., & Jung, H. (2019). Accounting for HIV health disparities: Risk and protective factors among older gay and bisexual men. Journal of Aging and Health. DOI: 10.1177/0898264319848570.
Emlet, C., Harris, L., Furlotte, C., Brennan, D., & Pierpaoli C. (2017). “I'm happy in my life now, I'm a positive person”: Approaches to successful ageing in older adults living with HIV in Ontario, Canada. Ageing and Society, 37(10), 2128-2151. DOI: 10.1017/S0144686X16000878.
Emlet, C., Tozay, S., & Raveis, V. (2010). “I’m not going to die from the AIDS’: Resilience in aging with HIV disease. Gerontologist, 51(1), 101-111. DOI: 10.1093/geront/gnq060.
Fang, X., Vincent, W., Calabrese, S.K., Heckman, T.G., Sikkema, K.J., Humphries, D.L., & Hansen, N.B. (2015). Resilience, stress, and life quality in older adults living with HIV/AIDS. Aging and Mental Health, 19(11), 1015-1021. DOI: 10.1080/13607863.2014.1003287.
Fergus, S., & Zimmerman, M.A. (2005). Adolescent resilience: A framework for understanding healthy development in the face of risk. Annual Review of Public Health, 26, 399–419. DOI: 10.1146/annurev.publhealth.26.021304.144357.
Flicker, S. Wilson, M., Travers, R., Bereket, T., McKay, C., Van der Meulen, A., Guta, A., Cleverly, S., & Rourke, S.B. (2009). Community-based research in AIDS service organizations: What helps and what doesn't?, AIDS Care, 21(1), 94-102. DOI: 10.1080/09540120802032650.
Genke J. (2004). Resistance and resilience: The untold story of gay men aging with chronic illness. Journal of Gay and Lesbian Social Service, 17, 81-95. DOI: 10.1300/J041v17n02_05.
Gigliello, J., & Ackerman, M.L. (2019). The issues of HIV stigma facing HIV positive gay men and how they cope through the mechanisms of resilience: A qualitative phenomenological transcendental study. Journal of AIDS and Clinical Research, 10, 1-8.
Gottert, A., Friedland, B., Geibel, S., Nyblade, L., Baral, S.D., Kentutsi, S., Mallouris, C., Sprague, L., Hows, J., Anam, F., Amanyeiwe, U., & Pulerwitz, J. (2019). The people living with HIV (PLHIV) resilience scale: Development and validation in three countries in the context of the PLHIV stigma index. AIDS and Behavior, 23(2), 172-182. DOI: 10.1007/s10461-019-02594-6.
Haddad, N., Robert, A., Weeks, A., Popovic, N., Siu, W., & Archibald, C. (2019). HIV in Canada - Surveillance Report, 2018. Canada Communicable Disease Report, 45(12), 304–312. DOI: 10.14745/ccdr.v45i12a01.
Halkitis, P.N., Krause, K.D., & Vieira, D.L. (2017). Mental health, psychosocial challenges and resilience in older adults living with HIV. Interdisciplinary Topics in Gerontology and Geriatrics, 42, 187-203. DOI: 10.1159/000448564.
Harper, G., Bruce, D., Hosek, S., Fernandez, M., Rood, B., & the Adolescent Medicine Trials Network for HIV/AIDS Intervention. (2014). Resilience processes demonstrated by young gay and bisexual men living with HIV: Implications for intervention. AIDS Patient Care and STDs, 28, 666-676. DOI:10.1089/apc.2013.0330.
Harrison, H., & Li, X. (2018). Rebooting resilience: Shifts toward dynamic, multi-level, and technology-based approaches for people living with HIV. AIDS Care, 30(5): S1-S5. DOI: 10.1080/09540121.2018.1557592.
Hart, T.A., James, C.A., Hagan, C.M., & Boucher, E. (2010). HIV optimism and high-risk sexual behaviour in two cohorts of men who have sex with men. Journal of the Association of Nurses in AIDS Care, 21, 439-443. DOI: 10.1016/j.jana.2010.06.001.
Herrick, A.L., Lim, S.H., Wei, C., Smith, H., Guadamuz, T., Friedman, M.S. & Stall, R. (2011). Resilience as an untapped resource in behavioral intervention design for gay men. AIDS and Behavior, 15, S25-S29. DOI: 10.1007/s10461-011-9895-0.
Herrick. A., Stall, R., Goldhammer, H., Egan, J., & Mayer, K. (2014). Resilience as a research framework and as a cornerstone of prevention research for gay and bisexual men: Theory and evidence. AIDS and Behavior, 18, 1-9. DOI: 10.1007/s10461-012-0384-x.
Hoover, K.W., Butler, M., Workowski, K., Carpio, F., Follansbee, S., Gratzer, B., Hare, B., Johnston, B., Theodore, J.L., Wohlfeiler, M., Tao, G., Brooks, J.T., Chorba, T., Irwin, K., Kent, C.K., & the Evaluation Group for Adherence to STD and Hepatitis Screening. (2010). STD Screening of HIV-Infected MSM in HIV Clinics. Sexually Transmitted Diseases, 37(12), 771-776. DOI: 10.1097/OLQ.0b013e3181e50058.
Huber, J.T. & Machin, M.S. (1995). Assessing the information needs of non-institutionally affiliated AIDS service organizations in Texas. Bulletin of the Medical Library Association, 83(2), 240-243.
Ibañez-Carrasco, F., Watson, J., & Tavares, J. (2019). Supporting peer researchers: recommendations from our lived experience/expertise in community-based research in Canada. Harm Reduction Journal, 16, 1-5. DOI: 10.1186/s12954-019-0322-6.
Ibañez-Carrasco, F., Worthington, C., Rourke, S.B., & Hastings, C. (2020). Universities without walls: A blended delivery approach to training the next generation of HIV researchers in Canada. International Journal of Environmental Research and Public Health, 17(12), 1-12.
Israel, B., Schulz, A., Parker, E., & Becker, A. (1998). Review of community-based research: Assessing partnership approaches to improve public health. Annual Review of Public Health, 19, 173–202. DOI: 10.1146/annurev.publhealth.19.1.173.
James, R. (2005). Building organisational resilience to HIV/AIDS: Implications for capacity building. Oxford, UK: INTRAC.
Kidder, D.P., Wolitski, R.J., Campsmith, M.L., & Nakamura, G.V. (2007). Health status, health care use, medication use, and medication adherence among homeless and housed people living with HIV/AIDS. American Journal of Public Health, 97(12), 2238-2245. DOI: 10.2105/AJPH.2006.090209.
Kidder, D.P., Wolitski, R.J., Royal, S., Aidala, A., Courtenay-Quirk, C., Holtgrave, D.R., Harre, D., Sumartojo, E., Stall, R., & the Housing and Health Study Team. (2007). Access to housing as a structural intervention for homeless and unstably housed people living with HIV: Rationale, methods, and implementation of the housing and health study. AIDS and Behavior, 11, S149-S161. DOI: 10.1007/s10461-007-9249-0.
Kurtz, S., Buttram, M., Surratt, H., & Stall, R. (2012). Resilience, syndemic factors, and serosorting behaviors among HIV-positive and HIV-negative substance-using MSM. AIDS Education and Prevention, 24(3), 193-205. DOI: 10.1521/aeap.2012.24.3.193.
Kwait, J., Valente, T.W., & Celentano, D.D. (2001). Interorganizational relationships among HIV/AIDS service organizations in Baltimore: A network analysis. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 78(3), 468-487. DOI: 10.1093/jurban/78.3.468.
Landers, S., Pickett, J., Rennie, L., & Wakefield, S. (2011). Community perspectives on developing a sexual health agenda for gay and bisexual men. AIDS and Behavior, 15, S101-6. DOI: 10.1007/s10461-011-9896-z.
Li, J., Gilmour, S., Zhang, H., Koyanagi, A., & Shibuya, K. (2012). The epidemiological impact and cost-effectiveness of HIV testing, antiretroviral treatment and harm reduction programs. AIDS, 26, 2069–2078. DOI: 10.1097/QAD.0b013e3283574e54.
Lincoln, Y., & Guba, E. (1985). Naturalistic Inquiry. Newbury Park, CA: Sage Publications.
Logie, C., James, L., Tharao, W., & Loutfy, M. (2013). Associations between HIV-related stigma, racial discrimination, gender discrimination, and depression among HIV-positive African, Caribbean, and Black women in Ontario Canada. AIDS Patient Care and STDs, 27(2):114–22. DOI: 10.1089/apc.2012.0296.
Luthar, S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71(3), 543–62. DOI: 10.1111/1467-8624.00164.
Marshall, B.D.L., Kerr, T., Shoveller, J.A., Patterson, T.L., Buxton, J.A., & Wood, E. (2009). Homelessness and unstable housing associated with an increased risk of HIV and STI transmission among street-involved youth. Health and Place, 15(3), 753-760. DOI: 10.1016/j.healthplace.2008.12.005.
Mayer, K.H., O’Cleirigh, C., Skeer, M., Covahey, C., Leidolf, E., Vanderwarker, R., & Safren, S.A. (2009). Which HIV-infected men who have sex with men in care are engaging in risky sex and acquiring sexually transmitted infections: findings from a Boston community health centre. Sex Transmitted Infections, 86, 66-70. DOI: 10.1136/sti.2009.036608.
McConnell, E.A., Janulis, P., Phillips, G., Truong, R., & Birkett, M. (2018). Multiple minority stress and LGBT community resilience among sexual minority men. Psychology of Sex Orientation and Gender Diversity, 5(1), 1–12. DOI: 10.1037/sgd0000265.
McNair, O.S., Gipson, J.A., Denson, D., Thompson, D.V., Sutton, M.Y., & Hickson, D.A. (2018). The associations of resilience and HIV risk behaviors among Black gay, bisexual, other men who have sex with men (MSM) in the deep south: The MARI study. AIDS and Behavior, 22(5), 1679-1687. DOI: 10.1007/s10461-017-1881-8.
Meyer, I.H. (2015). Resilience in the study of minority stress and health of sexual and gender minorities. Psychology of Sexual Orientation and Gender Diversity, 2(3), 209-213. DOI: 10.1037/sgd0000132.
O’Leary, A., Jemmott, J., Stevens, R., Rutledge, S., & Icard, L. (2014). Optimism and education buffer the effects of syndemic conditions on HIV status among African American men who have sex with men. AIDS and Behavior, 18, 2080-2088. DOI: 10.1007/s10461-014-0708-0
Paceley, M.S., Keene, L.C., & Lough, B.J. (2015). Motivations for involvement in nonmetropolitan LGBTQ organizations: A multimethod qualitative exploration. Journal of Community Practice, 23, 102–125. DOI: 10.1080/10705422.2014.985412.
Paceley, M.S., Keene, L.C., & Lough, B.J. (2016). Barriers to involvement in nonmetropolitan LGBTQ organizations. Journal of Gay & Lesbian Social Services, 28, 2, 117-139, DOI: 10.1080/10538720.2016.1155518.
Paterson, B.L., Ross, S., & Gaudet, T. (2014). Motives for meaningful involvement in rural AIDS service organizations, AIDS Care, 26(5), 582-586, DOI: 10.1080/09540121.2013.843771
Poindexter, C.C. (2007). Management successes and struggles for AIDS service organizations. Administration in Social Work, 31(3), 5-28. DOI: 10.1300/J147v31n03_02.
Public Health Agency of Canada. (2013). Population-specific HIV/AIDS status report: Gay, bisexual, two-spirit, and other men who have sex with men. Ottawa, Ontario: PHAC.
Quinn, G.P., Sutton, S.K., Winfield, B., Breen, S., Canales, J., Shetty, G., Sehovic, I., Green, B.L., & Schabath, M.B. (2015). Lesbian, gay, bisexual, transgender, queer/questioning (LGBTQ) perceptions and health care experiences. Journal of Gay and Lesbian Social Services, 27(2), 246-261. DOI: 10.1080/10538720.2015.1022273.
Rhodes S.D., & Wong F.Y. (2016). HIV prevention among diverse young MSM: Research needs, priorities, and opportunities. AIDS Education and Prevention, 28(3), 191-201. DOI: 10.1521/aeap.2016.28.3.191.
Rose, V.J., Raymond, H.F., Kellogg, T.A., & McFarland, W. (2006). Assessing the feasibility of harm reduction services for MSM: The late-night breakfast buffet study. Harm Reduction Journal, 3(29), 1-8. DOI: DOI: 10.1186/1477-7517-3-29.
Rossman, K., Salamanca, P., & Macapagal, K. (2017). A qualitative study examining young adults’ experiences of disclosure and nondisclosure of LGBTQ identity to health care providers. Journal of Homosexuality, 64, 1390-1410. DOI: 10.1080/00918369.2017.1321379.
Rounds, K., McGrath, B.B., & Walsh, E. (2013). Perspectives on provider behaviors: A qualitative study of sexual and gender minorities regarding quality of care. Contemporary Nurse, 44, 99-110. DOI: 10.5172/conu.2013.44.1.99.
Roy, C.M., & Cain, R. (2001). The involvement of people living with HIV/AIDS in community-based organizations: Contributions and constraints. AIDS Care, 13(4), 421–432. DOI: 10.1080/09540120120057950.
Sinclair, V.G., & Wallston, K.A. (2004). The development and psychometric evaluation of the brief resilient coping scale. Assessment, 11(1):94–101. DOI: 10.1177/1073191103258144.
Singh, S., Ruiguang, S., Johnson, A.S., McCray, E., & Hall, I. (2018). HIV incidence, prevalence, and undiagnosed infections in U.S. men who have sex with men. Annals of Internal Medicine, 168(10), 685-694. DOI: 10.7326/M17-2082.
Solomon, P., O’Brien, K., McGuff, R., & Sankey, M. (2019). Living strategies for disability in men ageing with HIV in Ontario, Canada: a longitudinal qualitative study. BMJ Open, 9, 1-8. DOI: 10.1136/bmjopen-2019-031262.
Spies, G., & Seedat, S. (2014). Depression and resilience in women with HIV and early life stress: does trauma play a mediating role? A cross- sectional study. BMJ Open, 4, 1-7. DOI: 10.1136/bmjopen-2013-004200.
Stall, R., Mills, T., Williamson, J., Hart, T.A., Greenwood, G., Paul, J., Pollack, L., Binson, D., Osmond, D., & Catania, J.A. (2003). Association of co-occurring psychosocial health problems and increased vulnerability to HIV/AIDS among urban men who have sex with men. American Journal of Public Health, 93, 939-42. DOI: 10.2105/ajph.93.6.939.
Stewart, M., Reid, G., Buckles, M., Edgar, W., Mangham, C., Tilley. N., & Jackson, S. (1999). A study of resiliency in communities. Ottawa, Canada: Health Canada.
Thurston, I.B., Howell, K.H., Kamody, R.C., Maclin-Akinyemi, C., & Mandell, J. (2018). Resilience as a moderator between syndemics and depression in mothers living with HIV. AIDS Care, 30, 1–8. DOI: 10.1080/09540121.2018.1446071.
Torres de Carvalho, F., Araujo de Morais, N., Koller, S.H., & Piccinini, C.A. (2007). Protective factors and resilience in people living with HIV/AIDS. Cad Saude Publica (Public Health Notebooks), 23(9), 2023-2033. DOI: 10.1590/s0102-311x2007000900011.
Trapence, G., Collins, C., Avrett, S., Carr, R., Sanchez, H., Ayala, G., Diouf, D., Beyrer, C., & Baral, S.D. (2012). From personal survival to public health: community leadership by men who have sex with men in the response to HIV. Lancet, 380, 400–410. DOI: 10.1016/S0140-6736(12)60834-4.
Travers, R., Wilson, M.G., Flicker, S., Guta, A., Bereket, T., McKay, C., Van der Meulen, A., Cleverly, S., Dickie, M., Globerman, J., & Rourke, S.B. (2008). The greater involvement of people living with AIDS principle: Theory vs. practice in Ontario’s HIV/AIDS community-based research sector. AIDS Care, 20(8), 615-624. DOI: 10.1080/09540120701661690.
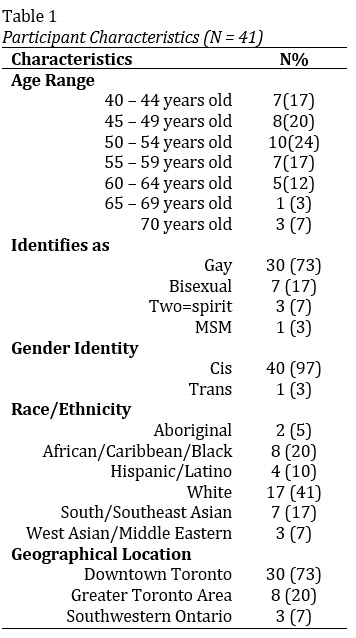 Table 1. Participant Characteristics (N = 41) |
 Renato M. Liboro, Tammy C. Yates, Charles Fehr, George Da Silva, Francisco Ibañez-Carrasco, Andrew D. Eaton, Daniel Pugh, Lori E. Ross, and Paul A. Shuper
Renato M. Liboro, Tammy C. Yates, Charles Fehr, George Da Silva, Francisco Ibañez-Carrasco, Andrew D. Eaton, Daniel Pugh, Lori E. Ross, and Paul A. Shuper
Renato (Rainier) M. Liboro, MD, PhD, is an Assistant Professor of the Department of Psychology of the University of Nevada, Las Vegas (UNLV), USA, and a Collaborator Scientist of the Institute for Mental Health Policy Research of the Centre for Addiction and Mental Health, Toronto, Canada. He is also the Director of the Community Health Advocacy for Minority Populations, Immigrants, and Other Newcomers, and their Mental Health (CHAMPION Mental Health) research lab at UNLV, and the Academic Research Involvement and Engagement Liaison of the LGBTQ Center of Southern Nevada. His community-based participatory research focuses on health disparities that impact the mental health and wellbeing of racial/ethnic and sexual/gender minorities, newcomers, older adults, and people living with HIV/AIDS and other hidden/episodic disabilities.
Tammy C. Yates, is the Executive Director of Realize, which hosts the Secretariat of the National Coordinating Committee on HIV and Aging, as well as the National Community Advisory Group on Optimal Health and Wellbeing in HIV. In 2015, Tammy became the first black female Executive Director of a national organization in Canada’s HIV response, as well as among Canada’s national disability organizations. She has worked for over fifteen years in the field of program management. Prior to joining Realize, Tammy was the National Program Manager of the United Nations Population Fund (UNFPA) - Trinidad and Tobago Branch Office. She has extensive experience in Gender and Development, and Sexual and Reproductive Health, including HIV/AIDS, having worked previously as a Program Officer with the Secretariat of the Caribbean Regional Network of Persons Living With HIV (CRN+), and served as Chair of the Gender Theme Group of the United Nations System in Trinidad and Tobago. She is a graduate of Wolfson College, Cambridge University, England, and the University of the West Indies, St. Augustine, Trinidad.
Charles Fehr, is currently a Research Assistant at the Institute for Mental Health Policy Research at the Centre for Addiction and Mental Health, working as a peer researcher for the "Older and Tougher: GBMSM Resilience Against HIV/AIDS" project. He has a Masters in Applied Social Psychology where he focused on the effects of prejudicial attitudes and behaviors on members of the LGBTQ community within the context of the workplace. He has previous experience conducting needs assessments and evaluations of student and health services. Charles is a member of the Re:Searching 2SLGBTQ+ Health team at the Dalla Lana School of Public Health of the University of Toronto. He has also worked as a coordinator facilitating research on GBMSM health with the CRUISElab team at Factor Inwentash, Faculty of Social Work of the University of Toronto. Charles is interested in continuing to pursue research on 2SLGBTQ+ health outcomes and working in research administration.
HIV-positive for over 20 years, George Da Silva, has been a peer researcher since 2017 and a dedicated volunteer in the community for a very long time. He became a peer researcher so that he could share and utilize his own lived experiences, as well as listen and learn from others’ stories. He has been involved in numerous research projects that have been conducted through the Centre for Addiction and Mental Health, Realize, the MAP Centre for Urban Health Solutions of St. Michael’s Hospital, and the University of Toronto. These research projects have focused on a wide range of topics from HIV/AIDS to homelessness.
Francisco Ibanez-Carrasco, PhD is an Assistant Professor at the Dalla Lana School of Public Health, University of Toronto, a member of The Canada-International HIV and Rehabilitation Research Collaborative (CIHRRC) and a fiction/non-fiction author. His research focuses on physical and cognitive rehabilitation in the context of HIV, queer men’s sexual health, eLearning for public health, HIV stigma, and autopathography (patient-oriented medical narratives).
Andrew D. Eaton, PhD is an Assistant Professor at the University of Regina’s Faculty of Social Work, Saskatoon Campus. His research focuses on addressing complexities of living and aging and HIV/AIDS, including interventions to alleviate the burden of cognitive impairment and peer support to ease hospital discharge. His research has received funding from the Canadian Institutes of Health Research (CIHR), the CIHR HIV Trials Network (CTN), and the Ontario HIV Treatment Network (OHTN). He is an OHTN Endgame Leader. He completed his PhD and Master of Social Work at the University of Toronto.
Daniel Pugh, MSW, is a registered social worker, psychotherapist, and mental health clinician at Casey House, the first and only stand-alone hospital for people living with HIV/AIDS in Toronto, Ontario, Canada. He completed his Master of Social Work from the University of Toronto - Factor Inwentash Faculty of Social Work in 2015. As a clinical social worker and mental health professional, he is eager to refine a practice that is trauma informed, anti-oppressive, sex-positive, decolonized, and rooted in harm reduction. He incorporates and affirms these values into his practice as a result of engaging in theory and practice with clients, community, peers, colleagues, and evidence.
Lori E. Ross, PhD, is an Associate Professor in the Division of Social and Behavioural Health Sciences, Dalla Lana School of Public Health, University of Toronto. She is an established interdisciplinary scholar in the field of sexual and gender minority (2SLGBTQ+) health. Her current program of research focuses predominantly on qualitative and mixed methods investigations of health determinants and experiences for diverse members of the 2SLGBTQ+ communities, as well as developing and evaluating interventions to address identified disparities.
Paul A. Shuper, PhD, is a Senior Scientist and Section Head in the Institute for Mental Health Policy Research at the Centre for Addiction and Mental Health in Toronto, Ontario, Canada. His research focuses on identifying and addressing the impact of addictions and mental health concerns on the prevention and treatment of infectious diseases, particularly HIV. Some of his current initiatives in this area include 1) an NIH/NIAAA-funded RCT that seeks to improve HIV pre-exposure prophylaxis (PrEP) treatment outcomes among gay and bisexual men by addressing underlying hazardous alcohol consumption, substance use, and depression through a brief e-intervention; 2) a CIHR-funded initiative that examines alcohol’s impact on the pronounced HIV and TB epidemics among mineworkers in South Africa; and 3) a CIHR-funded initiative that seeks to identify means of addressing alcohol, substance use, and mental health concerns among youth living with HIV in Zimbabwe. Based on his program of research, Dr. Shuper has served as a scientific expert in the area of alcohol and HIV for the World Health Organization. In January 2020, Dr. Shuper received an Ontario HIV Treatment Network “Innovator” Award for his work in the field of HIV.
agregar comentario
![]() Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
palabras clave: community-level resources, resilience, HIV/AIDS, middle-aged and older, men who have sex with men
 Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.
Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.

{kind=link}