The article provides the results, as well as policy and practice implications of an exploratory study on the feasibility and unique (unintended) benefits of surf therapy for children with Autism Spectrum Disorder (ASD), in a developing world context. The main aim of the study was to understand if and how Waves for Change (W4C), a South-African-based non-government organisation’s existing surf therapy programme for neuro-typical children can be adapted to be more inclusive and meet the needs of neuro-diverse children. The objective of the study was two-fold: 1) to gain an in-depth understanding of children’s experiences participating in surf therapy, with specific reference to confidence and self-identity; peer and adult relationships and connectedness; and communication initiation and verbal output; and 2) to understand if and how the existing W4C surf therapy model (designed with and for neuro-typical children) can be offered to a more diverse target population. The study found that children with ASD’s experiences at W4C’s surf therapy programme were predominantly positive and surf therapy can have a positive effect on children with ASD’s overall wellbeing. The research produced several suggestions for adaptations to the original W4C surf therapy programme, to be more appropriate and effective for neuro-diverse children and more specifically children with ASD.
Download the PDF version to access complete article, including Tables and Figures.
Introduction
Autism Spectrum Disorder (ASD) is recognized as a global public health concern, yet almost everything we know about ASD comes from high?income countries (Franz, Chambers, Von Isenburg & De Vries, 2017). As with most other intellectual and developmental disabilities, ASD occurs in every nation of the world, with families often providing lifelong care to their affected relatives. Unfortunately, in less affluent countries such as South Africa, there is a dearth of studies to inform the development of support services (Samadi & McConkey, 2011).
Results from a South African Stress and Health Survey (SASH) (Williams, Herman, Stein, Heeringa, Jackson, Moomal & Kessler, 2008) showed a 75% treatment gap of common mental disorders nationally. In addition to other factors that may be responsible for this treatment gap, stigmatisation of people with mental illness especially by health care professionals may also be responsible for this treatment gap (Jameson, 2006). It is evident that there is an increasing demand for mental health care in South Africa (as in most developing countries). There are only 1.12 psychiatrists, 1.28 psychologists and 1.6 social workers per 400,000 people in South Africa. Of the 23 mental hospitals in the country, only 18 (mental health) beds are allocated per 100,000 people. In addition, South Africa is a country where poverty is a real problem, and many people in the country live below the poverty line. Of the mental health professionals and services available in South Africa, most are based in urban areas, highlighting that mental health services are out of reach to the majority of South Africans who live in rural communities. As mental health services are predominantly limited to white middle-class individuals, many people living in poverty do not have the financial means to seek professional help (Cosme, 2015). The need for mental health care for differently-abled children appears to be even bigger than that of adults. In South Africa in 2013, there were 116,504 learners in the Special Need schooling sector who attended 448 institutions and were served by 10,252 educators (Republic of South Africa Departments of Social Development, and Women, Children and People with Disabilities, and The United Nations Children’s Fund [UNICEF], 2012). Under the Children’s Act (2007), the South African government is responsible for ensuring that comprehensive social services are provided for children, with priority being given to funding of services in poor communities, and to ensure that these services are accessible to children with disabilities. However, although non-government organisations (NGOs) are rendering services which are mandated by the Act, funds paid to them do not cover the full cost of providing these services. NGOs working in the disability sector have expressed grave concerns regarding accessing government funding. In South Africa, an excess of two million children (aged naught to 14) have some form of disability, including seeing (even when wearing glasses), hearing (even with a hearing aid), walking a kilometre or climbing stairs, remembering/concentrating, self-care such as washing or dressing, and communication in usual language including sign language (Republic of South Africa Departments of Social Development, and Women, Children and People with Disabilities, and UNICEF, 2012).
It is against this backdrop that W4C, a South African-based non-government organisation, has implemented and subsequently explored the feasibility and unique (unintended) benefits of its surf therapy programme to children with ASD.
Research Method
Study setting
The study was conducted over a 4-month period, at W4C’s existing surf therapy programme for children with ASD. While W4C has been in existence since 2011, their programme targeted neuro-typical children only. Since 2018, W4C have been piloting surf therapy with neuro-diverse children, such as children with ASD, in order to establish whether their service was appropriate to a more diverse target population. While W4C’s surf therapy programme for neuro-typical children followed a structured 16-week curriculum, the ASD pilot programmes were offered in a less structured way, informed by surf mentors’ informal observations and intuition of ‘what worked’ and ‘what didn’t work’ (things like communication barriers and children’s diverse cognitive abilities and needs, meant that surf mentors could not follow the existing structured 16-week surf therapy curriculum as they normally would). However, in order to formalise and/or scale a more inclusive surf therapy programme, formal research had to be conducted and used to inform such processes. During the 4-month research period, surf mentors offered the existing W4C 16-week surf therapy curriculum as best as possible, while researchers gathered data to establish more formally what worked and what didn’t, and what adaptations were required to the existing programme. Some adaptations were made and piloted during the 4-month period (these are discussed later).
Design
A qualitative, case study design (exploratory in nature) was used for this research.
Sample
The study population consisted of 45 children (5 female and 40 male children) (aged 13 to 17) diagnosed with ASD from two schools in the Western Cape, South Africa; who were all (at the time of the research) already participants in the W4C ASD surf therapy programme. Purposive sampling was done for the study, as all children that were in the programme at the time of the research (n=45), were purposely selected for data collection and inclusion in the study. The children were all in different areas on the Autism spectrum and therefore had a variety of abilities and needs. For example, some of the children were verbal, while others were pre-verbal; and some showed the cognitive ability to understand activities explained verbally by surf mentors, while others’ showed the cognitive ability to follow instructions through copying the behaviour and actions of surf mentors.
Data collection
While data collection was predominantly qualitative in nature, a mixed-methods data collection approach was used for the study. Qualitative data was collected through: a) focus group discussions (FGD) with 10 parents/caregivers, as well as 6 teachers and Occupational Therapists (FGDs were conducted at the end of the 4-month pilot surf therapy programme); b) surf mentor observations during surf therapy sessions (these were collected on an ongoing basis from the beginning to the end of the 4-month programme); and c) while both qualitative and quantitative data was collected through ‘on-the-beach’ feedback activities that gave children the opportunity to share their experiences of the programme using appropriate, inclusive tools, such as Makaton[1] (these were collected on an ongoing basis from the beginning to the end of the 4-month programme). Six Makaton symbols were displayed on surf mentors’ wetsuits, that children could point to, or read, or show using the relevant gesture. The Makaton symbols included ‘frightened’, ‘sad’, ‘angry’, ‘happy’, ‘calm’ and ‘brave’. Children were asked at three points during a surf therapy session how they felt while at W4C, which were pre-session (upon arrival at the programme), mid-session (after the ‘breathing/meditation activity’ on the beach), and post-session (once they have finished surfing or swimming in the ocean). In addition, if children did not point to or indicate any of the six symbols, ‘nothing’ was recorded. In some instances, children copied the surf mentor and did not provide a specific answer when asked how they felt; in which instances ‘copied’ was recorded. Lastly, children could also give any other answer in addition to the six Makaton symbols (if they wanted and were able to), which were recorded accordingly.
Data analysis
Researchers employed thematic data analysis to elicit key themes across all qualitative data collected from children, parents, teachers and surf mentors. In addition, frequency analysis methods were used to analyse quantitative data collected from children using Makaton.
The Waves for Change Surf Therapy Model
W4C provides a child-friendly mental health service to at-risk, vulnerable young people living in under-resourced, volatile communities. By fusing the rush of surfing with an evidence-based mind-body therapy curriculum, W4C helps children to develop skills to cope with chronic trauma, regulate emotions and behaviour, as well as develop a sense of purpose, belonging and belief. The programme is delivered by unemployed (and in most cases unskilled) youth, who are based in the communities where programme participants are referred from. These youth are employed on a two-year surf coach and mentor learnership at W4C; where they receive the appropriate training to facilitate the W4C curriculum. Children who have experienced repeat trauma (including violence, abuse and neglect) are referred to W4C through schools, as well as community and government referral partners (such as community-based organisations and Departments of Health and Social Development). Once enrolled at W4C, children participate in a 12-month surf therapy programme, which consists of weekly 3-hour sessions at the beach, where children not only learn to surf, but are connected to surf mentors who offer a 16-week coping skills curriculum. Over the 12-month period, children repeat the curriculum twice (to increase dosage and programme exposure). A typical 3-hour session consists of: a) an energiser/warm-up activity, with some physical exercise (such as a short run), followed by b) a group check-in (where children have an opportunity to share how they are doing and how they practised the skills they learnt the previous week, in the current week), c) a breathing/meditation activity, which includes a teachable moment (where coping skills are learnt), d) a surf lesson, where children also practice the coping skills taught (for example, trust, communication, breathing), and e) the day’s session is completed with a group debrief on the children’s experiences of the day’s session.
Research Findings
As per the purpose of this study, the findings are accordingly presented in two sections. Firstly, the short-term programme outcomes and unique (unintended) benefits of surf therapy for children with ASD will be explored first. Here, the findings of using Makaton in an attempt to capture children’s voices as to how they experienced surf therapy will also be provided. Secondly, learning on if and how the W4C surf therapy programme can be inclusively offered to neuro-diverse children, in a low-resource setting.
Short-term programme outcomes
Children with ASD struggle with behaviours like those that children who are not on the spectrum struggle with, even if the cause is different and the behaviours might be more extreme. Such behaviours may include (amongst others) low self-esteem, social interaction, communication, as well as hyper-sensitivity (for example to sounds and touch) (Autism Spectrum Australia, 2019). In addition, Children with ASD may have difficulties forming and maintaining meaningful relationships with others, as well as their peers (Reichow & Volkmar, 2009). These difficulties can lead to social isolation and can impact their social, emotional and cognitive development, academic achievements, as well as their self-esteem (Stuhl & Porter, 2015). Short-term outcomes of W4C’s surf therapy programme for neuro-typical children include increased self-esteem, improved peer and adult relationships, and decreased anti-social behaviour (such as violent behaviour and engagement with gangs) (Waves for Change, 2019). The current study aimed to explore whether children with ASD experienced the same and/or unique/unintended benefits from W4C’s surf therapy, with specific focus on their confidence and identity, peer and adult relationships, as well as communication initiation and verbal output.
Confidence and sense of identity
At W4C it is believed that attempting a challenging new task and facing fears in a supportive and safe environment builds confidence and resilience. By trying something new in a safe environment, children push their comfort zones and learn new abilities in themselves. Observations from W4C surf mentors supported this believe:
“A highlight was when W4C mentor Luxolo, who had been working patiently and in a structured way with two learners who were scared to get their faces wet, got them to kneel down in the water, and all together splash their faces. By the end of the session, the children were soaked and stoked!” - W4C surf mentor.
In addition, while children with ASD often appear to hold this perceived ‘disability’ as their master identity (which may make them experience some feelings of exclusion, marginalisation and discrimination), it was found that they developed a ‘new’ or ‘additional’ identity and sense of belonging in a (often perceived) unlikely group, being a surfer! In the first sessions of the W4C surf therapy curriculum, children learn how to be bananas. ‘Bananas’ is the W4C culture, and it means protecting each other from harm, respecting each other’s feelings, and communicating with each other about our feelings. The ‘bananas’ culture at W4C is visualised by the surfer ‘shaka’ sign (Figure 1; to see Figure 1, download the PDF version to access the complete article, including Tables and Figures).
“The W4C ‘bananas’ shaka sign is great for the children, as they respond well to ritual and structure. At school, children who never used to really interact with me will give the ‘bananas’ sign whenever they see me, which means they're associating me, that sign, and surfing together.” - Teacher and occupational therapist.
Peer and adult relationships
The W4C surf therapy curriculum incorporates numerous group and peer interaction activities. For example, pair floating and pair surfing, where participants team up in pairs or small groups and learn how to float and surf together. Through helping and teaching each other, children learn how to share and be patient. Children master how to share with each other, and to praise each other’s efforts.
“I have seen so many changes – self-confidence, communication and social interaction. In general children with their cognitive functions are quite independent and don’t do much group play or interaction. Since being at Waves for Change, the children have shown a willingness to engage with each other, build friendships and high fives…lots of high fives!” - Teacher.
“The children are more social at W4C than at school. Empathy, and understanding that someone else's feelings can be different to their own, is difficult for them. At the programme, they've shown a little more willingness to engage with each other, and to act as a group, which is great.” - Teacher.
Communication initiation and verbal output
While not every child with ASD has a language problem, a child’s ability to communicate will vary, depending upon his or her intellectual and social development (National Institutes of Health, 2012). While most of the children with ASD in the W4C surf therapy programme were unable to speak, some appeared to have a rich vocabulary and were able to talk about specific subjects in great detail. Most participants, however, had difficulty using any spoken language effectively to communicate with their surf mentors at W4C. While the W4C surf therapy programme does not aim to teach children with ASD to speak, a short-term outcome appeared to have been that there was an increase in children initiating communication (whether verbally or nonverbally using for example Makaton) and/or verbal output (such as increased participation in energisers using sounds).
“Introducing the W4C Kilo – a ‘follow-the-leader’ style group energizer, performed in a circle – also proved effective and increased the learners’ attempts to communicate with the W4C surf mentors. Call and response, copying actions and group activities were good for the learners. The learners were initially very independent and didn’t interact with the coaches easily. But this changed when they did the W4C kilo exercise.” - W4C surf mentor.
“One of the boys doesn't usually greet anyone. Last week, he specifically said hello to me though, and the teachers noticed and commented that it's something new for him to communicate in that way." - W4C surf mentor.
Unique/unintended benefits
Coping in new/unpredictable environments (other than school and home)
Sinha, Kjelgaard, Gandhi, Tsourdies, Cardinaux, Pantazis, Diamond and Held (2014) write that children with ASD experience the world as overwhelming, as they have difficulty predicting situations, which may increase anxiety and extreme sensory sensitivities. Neil, Olsen and Pellicano (2016) note that helping children who have ASD cope with uncertainty could ease some of these symptoms. This research made similar findings. A W4C surf mentor noted:
"These children need routine and structure. For two weeks there were roadworks between the school and the W4C beach programme, and the school bus had to take a different route. One of the young girls would cry and have aggressive outbursts, and only stop crying when they arrived at the W4C site. We thought this meant she thought they weren't coming, and got upset at the change in routine. It meant she's come to count on W4C as part of her structure and routine, and something she looked forward to." - W4C surf mentor.
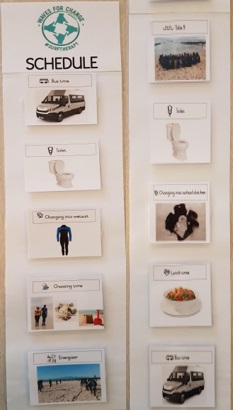
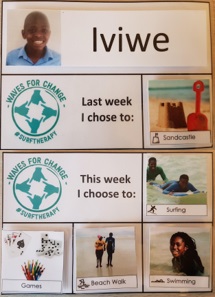
One of the major observed challenges children with ASD who participated in W4C’s surf therapy programme faced, was the negative effect any unforeseen changes in programme sessions had on participants. In general, when something unpredictable happened (for example, a session had to be cancelled or changed due to bad weather or community violence) the situation could be explained verbally to neuro-typical children and a session could either be cancelled or changed, without serious negative effects or harm caused to participants. However, when this happened during sessions with children with ASD, some participants displayed high levels of anxiety, anger and negative outbursts, and overall negative experiences during participation at W4C. When revised approaches to communicating, explaining and involving participants in unpredictable and unexpected situations were developed and followed, positive outcomes were observed. For example, a visual tool was developed and implemented to non-verbally articulate, but also make provision for unexpected changes in the programme structure and prepare children for such changes before they occur. This appeared to have helped children to cope better in unexpected situations when they attend the W4C surf therapy programme:
“It happened often that participants will come to the programme, but then it rained and we couldn’t take children to the beach to surf and we also couldn’t explain verbally to the children why we have to do something else, like play games or make art. Lots of the children then would get angry or upset and show behaviour that was not safe for themselves or the other children, like hitting or crying. This created a very difficult situation for us as coaches, as we didn’t want children to have a bad experience when they come to W4C. Since we implemented a visual tool, where children are prepared by teachers and us coaches, that they will have options of activities to choose from when they are at W4C, we found we could manage their expectations better and help them cope better in unexpected situations and changes in the programme sessions. On days where we couldn’t take the children to the beach for surfing, we removed that as an option for them to choose before they arrived at programme, leaving only non-beach activities for them to choose from. It was amazing to see how much better the children coped when they were prepared in a ‘language’ they understood for unpredictable situations and it looked like they started learning how to be okay with unexpected situations!” - W4C surf mentor.
In addition, some parents and teachers reported that some of the children were never able to go to environments other than home and school, as they were faced with unfamiliar and unpredictable situations and experiences. However, it appeared that their participation at W4C has assisted them to develop initial coping skills to visit other places, such as shopping malls, without experiencing the same amount of anxiety as previously.
Coping with sensory sensitivity (e.g. sand, water, wetsuit, dog/people on the beach)
One of the major challenges faced and raised by parents and teachers of children with ASD is that they were likely to be oversensitive to information they receive via their senses, such as noise, light, feeling or temperature.
“When the school contacted me to obtain my permission for my child to join W4C’s surfing programme, I thought that would be impossible! That is the sea...it is water! There is sand and wetness and fish and sharks. There are dogs and other people on the beach and my child has fears for all these stimuli.” - W4C participant parent.
The research found that most children with ASD who participated in the W4C surf therapy programme, gradually started to develop coping skills to regulate their sensory sensitivity while at W4C. Over time, children looked forward to putting their wetsuits on and feeling the water on their faces. A teacher reported that one of the children could not deal with feeling sand under her feet and would “hop from desk to desk and chair to chair” in the school classroom to avoid touching the ground, but after spending time at W4C the child became used to the beach sand under her feet and wear sandals to school on days she attends the W4C programme, as she did not mind feeling the sand under her feet anymore and looked forward to taking her sandals off at the beach. The W4C surf therapy programme provided children with ASD the opportunity to be exposed to sensory stimuli outside their home and school environment, in a physical and emotional safe space. This appeared to have helped these children regulate their responses to sensory stimuli over a period of time.
“Whenever my child saw a dog, she would be so scared and scream...and it would take a long time for her to calm down. We didn’t think this would ever change. Since joining W4C, she seems to be dealing with dogs better (it must be because she sees dogs on the beach every week). She told me that she might want a puppy one day and she is even thinking of names for the dog. I could not believe this!” - W4C participant parent.
Strengthen skills for independence
One of the main challenges children with ASD face is living an independent life as a young person, but also into adulthood. A "normal", independent adult life may include basic life skills (using the toilet, dressing, eating); functional skills (taking a bus, navigating the cafeteria, home repair, responding to a medical emergency); leisure or recreational skills (going to the library or playing a group sport); employment or vocational skills (getting to work on time, interacting with co-workers, doing the job); and technology skills (using a computer or smartphone, purchasing an item online). The ability to live an independent life (especially as an adolescent and ultimately as an adult) was also one of the main concerns parents of the children in the W4C surf therapy programme, had for their children. While the development of independent living skills would require longer-term interventions, some parents and teachers observed initial short-term changes in participants that suggested the development of skills to function independently.
“My child never used to do any chores at home. I continuously try to teach him to help with the dishes and fold up his clothes. Since participating at W4C, I noticed my child washes his own dishes and packs away his clean clothes. I think this may be because m y child has to do this for himself at W4C, no one there assists him with these chores. I am grateful that he is learning some of the things he will need when he lives by himself one day.” - W4C participant parent.
Listening to children’s voices using Makaton
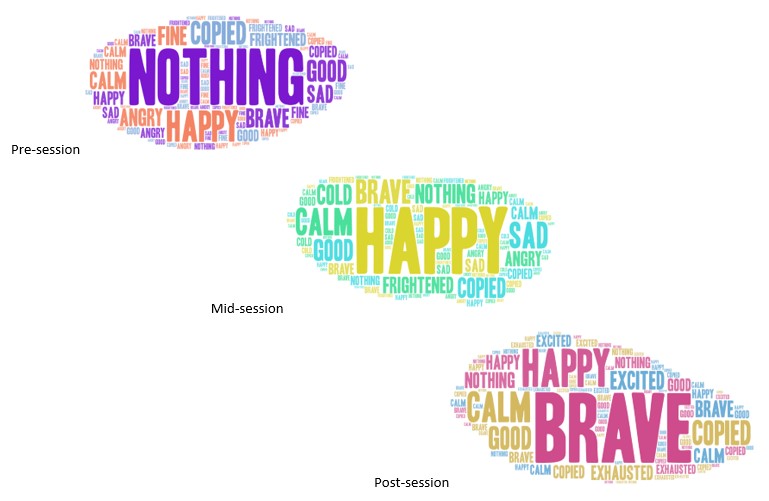
As mentioned earlier, one of the main barriers and concerns with the W4C surf therapy programme and its’ applicability to children with ASD, was the ability of children and surf mentors to communicate effectively. Of particular importance was the need for children with ASD to share how they feel at any given time during a surf therapy session. The use of Makaton as a communication method was piloted and the findings hereof are displayed below in word clouds[2].
Figure 1 (to see Figure 2, download the PDF version to access the complete article, including Tables and Figures) shows two important findings. Firstly, children most frequently did not indicate how they were feeling or did not select a Makaton symbol when they arrived for a session and before the session started; as ‘nothing’ (n=24) was most frequently recorded. In addition, other frequent responses from children before their surf therapy session started, included ‘happy’ (n=18), ‘sad’ (n=6), ‘angry’ (n=6), ‘brave’ (n=6), ‘good’ (n=5) and ‘frightened’ (n=5). The most frequent responses reported from children during a surf therapy session (after children completed a breathing/meditation/calming down activity) included ‘happy’ (n=28), ‘brave’ (n=15), ‘calm’ (n=10), ‘good’ (n=5) and ‘sad’ (n=4). Lastly, children reported most frequently to be ‘brave’ (n=24), ‘happy’ (n=19), ‘calm’ (n=13) and ‘excited’ (n=6) once they completed a surfing or swimming session in the ocean. From the above it can be interpreted that children’s experiences during a surf therapy session (in most instances) reflected they arrived at sessions less inclined to share how they were feeling and/or that they did not know how they were feeling. After completing a calming down/breathing/meditation activity, children (in most instances) appeared to be calm and happy; while after the surfing/swimming activity in the ocean, children experienced feelings of being brave, happy, calm and excited. Secondly, one of the main reasons for developing and using non-verbal communication tools, such as the Makaton wetsuit armbands, was to encourage and increase communication between surf mentors and participants, as well as to provide a platform where children with ASD’s voices can be heard (in cases where these children were pre- or non-verbal). When comparing the frequencies of ‘nothing’ and ‘copied’ used at the pre, mid and post-session data collection points, it was found that children more frequently did not initiate communication with their surf mentors when they arrived at a session, but that they appeared to be more inclined to initiate communication as the session progressed. This may allude to the possibility that these visual aids, as well as the trust and safe space being created between surf mentors and participants during a session, provided children with ASD with an opportunity to increase communication initiation, as well as to form meaningful relationships.
Feasibility of current W4C programme for inclusive surf therapy
Overall, it was found that W4C’s surf therapy programme can be offered as a meaningful, community-based mental health service to children with ASD. However, not in the format offered to neuro-typical children, as the programme in its current form was not optimally inclusive and appropriate for neuro-diverse children (such as those with ASD). Through working closely with Occupational Therapists and teachers at schools for children with ASD, some adaptations to the existing W4C surf therapy programme were made and briefly piloted during the research; which included:
Practice and Policy Implications
This research uncovered three main challenges (amongst others) faced by mental health services for children with ASD in a developing country, such as South Africa. Firstly, there is a dearth of research that informs a better understanding of ASD and subsequent guidance for appropriate mental health interventions. Secondly, accessible mental health services are far and few, with less than 5 qualified clinicians (such as social workers, therapists or psychologists) per 400,000 people in South Africa. Lastly, alternative and/or supplementary mental health programmes for children and young adults (such as W4C’s surf therapy programme) are often developed for neuro-typical children and involves ‘typical’ cognitive and physical functioning (such as verbal communication skills, understanding of spoken languages, and reading and writing). The research found that, despite these challenges, existing resources and programmes (such as W4C’s surf therapy programme) can be “re-worked” and implemented to fill some of the mental health service gaps for neuro-diverse children in low resource, developing settings. Some of the main recommendations derived from the research, that may be used to inform policy and practice in this context included:
Concluding Thoughts
ASD is an invisible disability. While individuals with, for example, a physical disability can be recognised by their use of a wheelchair, or the visually impaired by their use of a guide dog, there are no definite signs that a person has ASD. This often results in limited understanding of people with ASD. People very often judge children with ASD as being naughty or as being defiant; this is not the case. It is because of their inability to understand social rules that others very often just accept as the social norm. People with ASD have difficulty interacting with others and communicating, their senses are sometimes impaired, and they have a rigid way of thinking. Children with ASD, specifically in developing countries, are excluded from almost all service provision in their communities and face challenges associated with stigma and discrimination, leading to isolation and poor mental and physical health. Community-based mental health services, such as the W4C surf therapy programme, can support neuro-diverse children to integrate coping strategies into their lives, practice socially appropriate behaviour, promote physical activity, as well as develop independent living skills. Through an adapted programme that promotes meaningful participation of this group, and specialist training for community-based programme facilitators, mental health services can be inclusive and support all young people to become independent and reach their potential. A need for further, longer-term research was identified, to probe both the longer-term outcomes of surf therapy for children with ASD, as well as the possible effect more inclusive programme delivery tools may have on children’s experiences while participating in W4C surf therapy programme.
Research Limitations
Some of the main research limitations for this study are listed below; which should also be considered during the interpretation of the study findings and subsequent conclusions:
Influence from the researcher: this is an inevitable limitation, due to the interaction between the researchers and participants in a social process. In addition, in this study, some of the researchers were employed at the programme explored in the study. As such, researchers were aware of personal bias, values and beliefs whilst conducting the research so as not to influence the results in any manner; and
Study design and length: this was a pilot study and exploratory in nature, over a limited four-month period, which restricted the nature and amount of data that could be collected, analysed and interpreted. More specifically, the study duration did not allow for newly designed programme tools (such as visual aids) to be rigidly evaluated; these tools were piloted and initial feedback on their suitability and potential to offer inclusive surf therapy were assessed and reported on. As such, the findings should be interpreted with caution.
References
Autism Spectrum Australia. (2019). Difficulty areas. Available from: https://www.autismspectrum.org.au/content/areas-difficulty.
Cavanaugh, L.K & Rademacher, S.B. (2014). How SURFing Social Skills Curriculum can Impact Children with Autism Spectrum Disorders. The Journal of the International Association of Special Education, Spring 2015, 15(1):17-27.
Clapham, E.D., Armitano, C.N., Lamont, L.S. & Audette, J.G. (2014). The Ocean as a Unique Therapeutic Environment: Developing a Surfing Program, Journal of Physical Education, Recreation & Dance, 85:4, 8-14
Cosme, G. (2015). Lack of mental health services in South Africa. Available from: http://www.ginocos.me/blog/lack-of-mental-healthcare-south-africa
Franz, L., Chambers, N., Von Isenburg,M., & De Vries, P.J.. (2017). Autism spectrum disorder in sub-saharan Africa: A comprehensive scoping review. Autism Res, 10: 723-749.
Jamison, K. R. (2006). The many stigmas of mental illness. Lancet. 2006, 367 (9509): 533-534.
National Institutes of Health. (2012). National Institute on Deafness and Other Communication Disorders (NIDCD) Fact Sheet ? Voice, Speech, and Language Communication Problems in Children with Autism Spectrum Disorder. Available from: https://www.nidcd.nih.gov/sites/default/files/Documents/health/voice/NIDCD-Communication-Problems-in-Children-with-Autism-FS_0.pdf.
Neil, L., Olsson, N.C. & Pellicano, E. (2016). The Relationship Between Intolerance of Uncertainty, Sensory Sensitivities, and Anxiety in Autistic and Typically Developing Children.
Pauw, I. (2011). The stigma of mental illness. Available from: https://www.health24.com/mental-health/living-with-mental-illness/the-stigma-of-mental-illness-20120721
Reichow, B., & Volkmar, F. (2009). Social skills interventions for individuals with Autism: Evaluation for evidence-based practices within a best evidence synthesis framework. Journal of Autism and Developmental Disorders, 40, 149–166.
Republic of South Africa Departments of Social Development, and Women, Children and People with Disabilities, and The United Nations Children’s Fund (UNICEF). (2012_. Children with Disabilities in South Africa: A Situation Analysis 2001-2011. Available from: https://www.unicef.org/southafrica/SAF_resources_sitandisability.pdf.
Sayyed Ali Samadi and Roy McConkey. (2011). Autism in Developing Countries: Lessons from Iran. Autism Research and Treatment Volume 2011.
Silver EB (1970). Operant conditioning of speech sounds in an autistic child. South African Journal of Psychology. 1970:3–12.
Sinha, P., Kjelgaard, M.M., Gandhi, T.K., Tsourides, K., Cardinaux, A.L., Pantazis, D. Diamond, S.P., Held, R.M. (2016). Autism as a disorder of prediction. J Autism Dev Disord. 2016 Jun;46(6):1962-1973
Stuhl & H. Porter. (2015). Riding the Waves: Therapeutic Surfing to Improve Social Skills for Children with Autism. Therapeutic Recreation Journal, XLIX(3):253-256.
Travis J, Geiger M. The effectiveness of the Picture Exchange Communication System (PECS) for children with autism spectrum disorder (ASD): A South African pilot study. Child Language Teaching & Therapy. 2010; 26:39–59.
UNICEF South Africa. (2019). Available from: https://www.unicef.org/southafrica/support_4707.html.
Waves for Change. (2019). W4C Impact. Retrieved from: https://www.waves-for-change.org/w4c-impact/
Williams D, Herman A, Stein D, Heeringa S, Jackson P, Moomal H, Kessler R. (2008).: Twelve-month mental disorders in South Africa: prevalence, service use and demographic correlates in the population-based South African Stress and Health Study. Psychol Med. 2008, 38 (2): 211-220.
[1] Makaton is a unique language programme using a systematic multi-modal approach of speech, signs and symbols to teach communication, language and literacy skills to people with communication and learning difficulties. Available from: http://www.makaton.co.za/page/what-is-makaton
[2] Word clouds are graphical representations of word frequency that give greater prominence to words that appear more frequently in a source text. The larger the word in the visual the more common the word was in the document(s).
 Nicci van der Merwe & Paula Yarrow
Nicci van der Merwe & Paula Yarrow
Nicci van der Merwe, holds a Masters degree in Programme Evaluation (University of Cape Town). She has 10 years’ quantitative and qualitative research experience in the development sector, which includes programme monitoring, evaluation and learning (MEL) experience.
Paula Yarrow, holds a degree in Sport and Exercise Science and a Bachelor of Laws (LLB), specialising in children's rights. She has 8 years of experience living and working with grassroots Non-Governmental Organisations (NGOs) in Eastern and Southern Africa, as well as South East Asia.
agregar comentario
![]() Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
palabras clave: surf therapy, mental health, Autism Spectrum Disorder, neuro-diverse, community-based
 Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.
Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.