The purpose of this study was to evaluate the benefits of participation in a one-day surf therapy program among youth at-promise. Participants (N=152) were predominantly Hispanic or Latino (71%), followed by Black or African American (18%), 57% were Female, and age ranged from 6 to 19 years. Participant drawings were rated to evaluate program process. The program outcome was evaluated through an observational one-group pretest-posttest follow-up design using the Children’s Hope Scale. A paired samples t-test found a statistically significant increase in mean scores on hope after participation. A one-way analysis of variance on a subsample (n=50) with one month follow up data found a statistically significant increase in mean scores on hope after participation and one-month after participation. Results suggest that the study participants experienced a significant increase in hope through their participation in the Jimmy Miller Memorial Foundation’s one-day ocean therapy program. Limitations of the study design and implications for research and practice are discussed.
Download the PDF version to access complete article, including Tables and Figures.
The population of Los Angeles County, California was just over 10 million in 2016, with a youth (0-18 years of age) population of nearly 2.5 million. The dominant ethnicity of youth in Los Angeles County is Latino (48.4%), followed by White (28.3%), Asian/Pacific Islander (14.6%), African-American (8.5%) and Native American (0.19%) (Los Angeles County Department of Mental Health, 2017). Nearly 40% (979,991) of these youth are estimated to be living at or below the 138% Federal Poverty Level, 8% are estimated to experience serious emotional disturbances or serious mental illness, and only about 3% of youth ages 0-15 were served by outpatient mental health programs in the 2015-2016 year (LACDMH, 2017). Of the estimated 30,000 youth in foster care in Los Angeles, less than 50% graduate from high school, 33% of young women become pregnant by age 17, 25% who age out of foster care will be incarcerated within two years, and, at age 19, 60% of former foster youth are unemployed (CASA, 2015). Furthermore, obesity among youth in Los Angeles has been found to be significantly related to economic hardship (Los Angeles County Department of Public Health, 2011) and rose nearly 5% among youth 12-17 years of age between 2001 and 2012 (Wolstein, Babey, & Diamant, 2015). These data are by no means comprehensive but provide a broad view of the prevalence of characteristics that are relevant to youth ‘at-promise’ in Los Angeles County.
In October 2019, the state of California passed legislation to amend language in the Education Code and replace the term at-risk with at-promise (Assembly Bill No. 413, 2019). The legislation also added language about the role of schools in developing policy and procedure to address intimidation, harassment, discrimination and bullying based on identity or status - immigration status, gender-identity/expression, disability, ethnicity, race, sexual orientation, religion, nationality, or association with a person or group. Youth in foster care and recipients of the public mental healthcare system are also identified as ‘at-promise’ due to socioeconomic disadvantage and exposure to trauma and other adverse experiences such as abuse, neglect or permanent separation from parents. The term at-promise was intended to acknowledge the resilience of youth growing up in challenging conditions and remove the negative stigma associated with the term at-risk (Assembly Bill No. 413, 2019).
Adverse experiences are traumatic experiences that affect the developing body and brain of a child, and, that may impact adult health and livelihood. Adverse experiences in childhood have been correlated to negative health behaviors and several leading causes of death in adulthood, including abuse (i.e., physical, emotional, sexual), neglect (i.e., physical and emotional) and household dysfunction (i.e., mental illness, incarcerated relative, mother treated violently, substance abuse, and/or divorce) (Felitti et al., 1998). In a study of 13,494 adults from a large Health Maintenance Organization (HMO), compared to respondents with zero adverse childhood experiences, respondents reporting four or more adverse child experiences had increased risks for drug/alcohol abuse, smoking, depression, suicidal attempts, sexually transmitted diseases and obesity (Felitti et al., 1998).
There is some research to suggest hope may strengthen resilience among youth at-promise. Hope among youth has been defined as cognitively based beliefs in the capability to take realistic steps to accomplishing goals and self-perceptions of one’s ability to begin and sustain movement toward goal attainment (Snyder et al., 1997). Hope among youth has been found to be positively related to life satisfaction, personal adjustment, higher academic achievement and greater participation in structured extracurricular activities (Gilman et al., 2006). Hope has also been found to be positively related to family cohesion and adaptability and negatively related to loneliness (Sharabi et al., 2012). Among youth at-risk, hope is believed to be a critical factor in resilience while the lack of hope is thought to impact individual vulnerability (Martinek & Hellison, 1997). Among a sample (N=699) of youth at-risk who were predominantly African-American and from low-income communities, Valle et al. (2006) found that high scores on hope not only predicted higher scores on life satisfaction a year later but also found that hope served as a moderator to stressful life events resulting in fewer maladaptive internalizing behaviors a year later, suggesting that hope can serve as a buffer to negative life events. These results suggest that hope may serve as a protective factor for youth at-promise experiencing stressful life events.
Outdoor water environments and surf therapy programs may provide opportunities for participants to increase hope through respite, social support and the physical activity of surfing. The use of outdoor water environments or blue space for the benefit of health and wellbeing has grown in recent years (Britton et al., 2018). Although many blue space activities including scuba diving (Carin-Levy & Jones, 20017), kayaking (Casey, O’Broin, & Collins, 2009) and river running (Dustin et al., 2011), have been explored, the sport of surfing specifically has demonstrated increases in multiple areas including positive affect and mood (Pittsinger et al., 2017), health and wellbeing (Britton, et al., 2018), physical strength, endurance and agility (Farley, Harris, & Kilding, 2018). Surfing is a unique sport that allows an individual to engage with nature in a symbiotic manner, whereby the individual not only physically propels them self into a wave, but must also connect their efforts to become part of the wave in a fluid manner. This fluidity gives way to the concept of flow or a state where a person performing an activity is fully immersed in the feeling of energized focus, full involvement, and enjoyment in the process of the activity (Czikszentmihalyi, 1990). Surfing provides a natural catalyst for the bi-products of wellbeing and self-efficacy to emerge.
Surf therapy is an emerging intervention technique for youth, which combines supportive surf instruction with group processing for the positive outcome of improved mental and physical health. From existing studies, psychological benefits of surf therapy have been shown to include increases in self-concept, emotional regulation and social competencies (Morgan, 2010; Taylor, 2013; Colpus & Taylor, 2014; Godfrey, Devine-Wrigtht, & Taylor, 2015); re-engagement with school (Matos, et al., 2017), and decreases in behavioral problems (Matos, et al., 2017; Morgan, 2010). Physical benefits included improvements in cardiovascular fitness (Hignett, et al., 2017), improved sleep (Morgan, 2010), higher levels of physical activity upon program completion and healthier choices as reported by parents of participants (Godfrey, et al, 2015). For youth with disabilities, parent-reported benefits have included increases in confidence and social skills, improvements in behavior (Armitano et al., 2015; Clapham et al., 2014; Moore, Clapham & Deeney, 2018; Mueller, 2017), opportunities for family bonding, and opportunities for normalizing for children who tend to be excluded from social events with their peers (Moore, Clapham & Deeney, 2017).
Although published results demonstrate positive benefits for youth, the duration of programs vary, ranging from 6 to 32 weeks. Most programs meet once or twice per week, totaling between 8 and 60 individual sessions. Research on one-day programs is rare and existing data from adult populations indicates that a one-day surf session can produce significant positive results (Pittsinger et al., 2017). Evidence indicates that a 30-minute surfing session could produce significant increases in positive affect and tranquility, regardless of the individual’s surfing history, frequency or pAaskill level (Pittsinger et al., 2017). The theme of escape or respite through the activity of surfing has emerged among adult populations in qualitative research among veteran populations with PTSD (Caddick et al., 2015). Participants from a qualitative study by Wheaton et al. (2017) described surfing as an unstructured freeing experience that promotes personal transformation as an alternative discourse to the dominant sports activity research perpetuating a value on achievement through structured activities to build individual and interpersonal skills. In the context of this research, and consistent with the flow state described above (Czikszentmihalyi, 1990), escape includes temporarily leaving everyday concerns behind through being in the ocean and experiencing the freedom of riding waves (Caddick et al., 2015; Wheaton et al., 2017).
While the benefits of participating in surf therapy programs have been observed, children’s hope has only been studied in one randomized control trial that found no significant differences in pretest-posttest scores between experimental and control groups or after participation in a 32-week, 64-session surf therapy program (Snelling, 2015). Study limitations included program attendance, in that participants attended less than half of the available sessions, and a prolonged period of time between testing in that the posttest was administered 32 weeks after the pretest (Snelling, 2015).
Program Description
The Jimmy Miller Memorial Foundation (JMMF) is a nonprofit 501c3 established in memory of Jimmy Miller, an exceptional waterman and ocean lifeguard who sustained a quick onset of mental illness and tragically took his own life shortly after receiving his diagnosis. Jimmy’s expansive community, along with his family, came together to create a non-profit that showcased Jimmy’s love for the ocean and surfing. The JMMF ocean therapy program was first implemented in 2005 to increase perceived self-efficacy and physical activity among youth at-promise through engagement with the ocean environment. Ocean Therapy is a “community-based, sports-oriented occupational therapy intervention,” which “combines surfing performance, focused group processing, and social participation” (Rogers, Mallinson & Peppers, 2014, p. 396). The program is designed to provide an inclusive and supportive social setting where participants can gain respite through experiencing the ocean and acquire new surfing skills in a safe but unpredictable ocean environment. The JMMF partners with organizations who serve youth in foster care, youth receiving individual and/or family therapy, and youth at-risk for negative outcomes in adulthood due to early traumatic experiences (e.g., exposure to individual, family or community violence).
The one-day ocean therapy program for youth at-promise includes 1) an opening talking circle where participants share their experience around a given theme, 2) a surf lesson on land, 3) a surf lesson in the ocean, 4) a second talking circle, 5) a second surf lesson in the ocean, 6) lunch, and 7) a closing talking circle with opportunity to reflect on the theme of the day and other experiences (e.g., about self, the ocean, or other attendees). Typically, there are 10-12 youth participants at each JMMF ocean therapy session and the program is free to participants. While the program is intended as a one-day program, participants have returned three or more times, especially participants who are affiliated with a JMMF partner organization for multiple years. In terms of surfing skills, the main goal of the program is for participants to be exposed to surfing in a fun, safe and socially inclusive environment. Ideally, participants are provided with a means of escape through exposure to the ocean and surfing with talking circles to provide space to express new perspectives that may have been gained through the day. During surf lessons, while riding a wave, participants are encouraged to move into a standing position on the board, with the instructor riding on the back of the board for support. Based on a participant’s experience with the ocean and surfing, skills such as paddling, balancing, sitting on the board, and surfing without the instructor on the back of the board may also be practiced. The surf lesson is participant-centered, so if interest is lost in surfing, alternative activities such as body surfing are available.
Through talking circles, participants experience an inclusive social environment where they can express feelings and share their life experiences. The talking circles focus on various themes, such as learning to face new challenges, allowing for participants, program surf instructors and volunteers to share their experiences in a socially inclusive environment. The ratio of surf instructors to participants is 1:1 and a water-volunteer assists participant-instructor dyads through retrieving surf boards and providing other assistance. An important aspect of safety to the JMMF model of surf-instruction is that instructors utilize a teaching method whereby they ride on the back of the board behind the participant all the way to the shore to provide maximum stability. Finally, there is an ocean safety coordinator at every session who is either an expert surf instructor or a former Los Angeles County ocean lifeguard, and, each session is facilitated by the program director who is a licensed therapist (i.e., licensed marriage and family therapist or occupational therapist).
Current Study
The current study reports on data collected during the summer 2017 and 2018 JMMF ocean therapy sessions. The program evaluation utilized a mixed-method approach employing qualitative methods to assess program process and quantitative methods to assess the program outcome. Program process was evaluated through rating participant drawings. The program outcome was evaluated through an observational one-group pretest-posttest-follow-up design. It was hypothesized that one of the benefits to participation in a one-day surf therapy program is a significant increase in hope.
Method
Participants
Participants were recruited through five JMMF partner, youth-serving organizations, two that chose to keep their names anonymous. Of the five partner organizations, two were mental health organizations (Didi Hirsch Mental Health Services & Richstone Family Center), two were youth summer camps providing services to youth in foster care or receiving mental health services (Happy Trails for Kids & Organization 4), and one was a group home for youth in foster care (Organization 5). All participants were either receiving public mental health services or in the foster care system or both. Partner organizations utilized differing inclusion criteria for participation in the JMMF ocean therapy program and all program participants were invited to participate in this study resulting in a convenience sample. While two partner organizations did not use any inclusion criteria other than participant availability, two organizations used recent prosocial behaviors (e.g., helping friends work out a conflict) and one used recent leadership behaviors (e.g., leadership in groups conducting project-based learning) exhibited by potential participants.
Qualitative data were collected from 157 participants and quantitative data were collected from 152 participants. Five participants opted out of completing quantitative data but completed qualitative data. Additionally, one-month follow-up data from a subsample of 50 participants with additional demographics on history of adverse experiences and personal challenges are included in this study. While participants do not participate in the program more than once a year, some participants have participated for multiple years if they are affiliated with the same JMMF partner organization. Thus, some data may reflect participants who have participated in multiple years of the program.
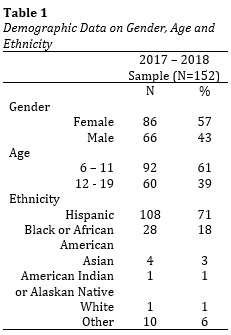
Table 1 (to see Table 1, download the PDF version to access the complete article, including Tables and Figures) presents demographic data on the main sample of 152 participants who completed quantitative questionnaires. Fifty-seven percent (n=86) were female and age ranged from 6 to 19 years (M age = 11.29). Two age categories are presented: 6-11 and 12-19, based on Piaget’s Stages of Cognitive Development, which associate these age ranges with the concrete operational and formal operational stages, respectively (Piaget, 1964). The ethnicity of participants was predominantly Hispanic or Latino (71%), followed by Black or African-American (18%) and Other Ethnicity (6%). Of the 10 participants who indicated an Other Ethnicity, six were Hispanic or Latino and White, one was Hispanic or Latino and Black or African American, one was Black or African American and Jamaican, one was Black or African American/Mixed, and one was Mixed.
Of the subsample of 50 participants with one-month follow-up data, age ranged from 8 to 19 years (M age = 12.24), 54% were Hispanic or Latino and 40% were Black or African-American. Based on the ACEs study (Felitti et al., 1998) and personal challenges faced by youth at-promise (Assembly Bill No. 413, 2019), demographic data on selected adverse experiences and personal challenges were obtained from therapists of participants when available. While the average number of adverse experiences and personal challenges was over 1.5 (M adverse experiences and/or personal challenges = 1.69, n=50), 70% had a history of Emotional or Behavioral Problems, 34% had a history of Trauma, 28% had a Learning Disability or Educational Difficulties, 26% experienced Child Abuse or Neglect and 10% had a history of Substance/Alcohol Use/Abuse.
Measures
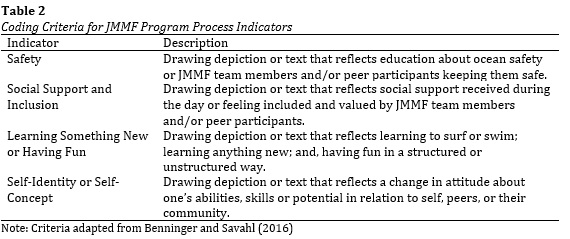
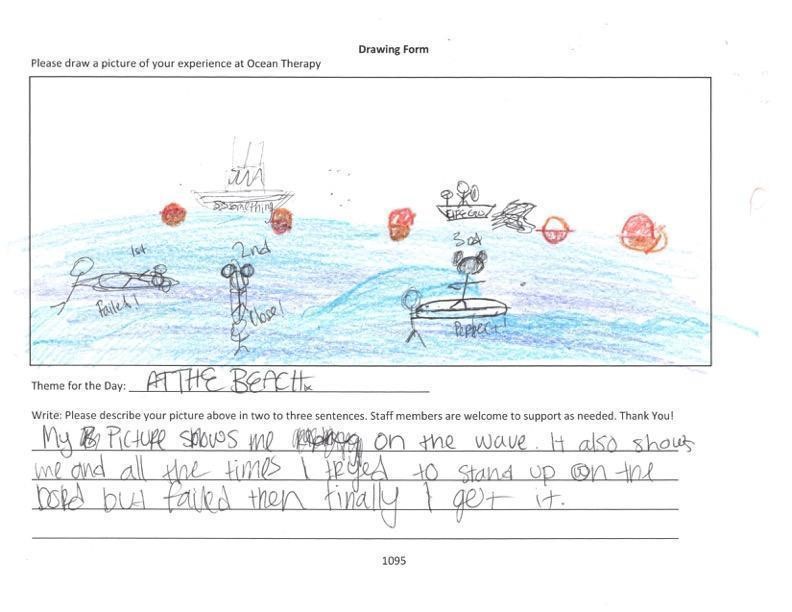
Drawing form. A drawing form was constructed by the first and third authors as an exploratory method of obtaining projective data on participants’ experience of the ocean therapy program. While the drawing form was used initially to identify potential outcomes of interest, it has been used to assess program process since 2017. Participants complete a drawing of their Experience of the Day and have space to write in a theme for the day as well as a few sentences to describe their drawing. While there is a theme in the talking circles during the ocean therapy session, participants are free to enter whatever theme they choose. Next, drawings and their associated text are rated based on a coding system developed from prior research by Benninger and Savahl (2016) that applied the Delphi method to identify aspects of social programs 10-12-year-old, impoverished youth in Cape Town, South Africa found to be most beneficial to their well-being – Children’s Safety, Social Support, Opportunities of Learning and Fun, and Basic Needs. These findings were adapted to reflect the JMMF ocean therapy program processes, developed into coding criteria and are described in Table 2 (to see Table 2, download the PDF version to access the complete article, including Tables and Figures). Drawings and their associated text were then rated for expression of the four program process indicators.
An inter-rater reliability analysis was conducted for both years in which a total of 157 drawings were rated. In summer 2017, three volunteers from JMMF served as primary raters with each rating all 73 drawings. In summer 2018, two volunteers (one from 2017 and one new) served as primary raters with each rating all 84 drawings. The primary author of this article served as the final judge in resolving discrepancies between raters for both years. Total inter-rater reliability was 32% (23 of 73 drawings coded the same on all four items) for 2017 and 57% (48 of 84 drawings coded the same on all four items) for 2018. The lower percentage for inter-rater reliability during 2017 is due in part to having three versus two raters. Both percentages were interpreted to have acceptable levels of inter-rater reliability for the number of raters.
Hope. Participants completed Snyder et al.’s (1997) Children’s Hope Scale, a six-item measure that defines hope as including pathways and agency as they relate to future goals, using the following statements measured on a Likert scale:
Hope is conceptualized as consisting of cognitive processes related to future goal attainment. Three items focus on agency, defined as beliefs about beginning and making progress toward goals, and three items focus on pathways, defined as belief in one’s capacity to develop realistic routes to accomplish goals.
The Children’s Hope Scale (Snyder et al., 1997) utilizes a six-point Likert scale with responses ranging from “None of the Time” to “All of the Time” and has been validated across five samples with youth 8 to 16 years of age with no statistically significant differences found on age, gender or between three ethnic groups (Hispanic or Latino, Black or African-American and White). In terms of internal consistency, Cronbach’s Alphas ranged from .72 to .86 with a median Alpha of .77. Temporal stability was reflected by strong correlations for a 1-month test-retest sample r(359)=.71, p<.001 and a 1-week test-retest sample r(89) =.73, p<.001. Convergent validity was established through statistically significant positive correlations to parent ratings of their children’s hope, children’s scores on competence, self-perception, and self-worth scales, and statistically significant negative correlations to perceived helplessness and depression.
Procedure
Institutional Review Board (IRB) approval was obtained from Antioch University Los Angeles in June, 2017. The only inclusion criterion was participation in the JMMF ocean therapy program. Parents of participants provided informed consent and participants provided assent. Staff from JMMF partner organizations were trained in the IRB-approved data collection protocol and collected all data.
Two to four weeks before each partner organization had their first ocean therapy session, the JMMF research team provided on-site training on the IRB-approved data collection protocol. The five partner organizations determined which potential participants were eligible to participate in the ocean therapy program. Parental informed consent and oral assent from participants was obtained by trained staff from partner organizations. Staff from partner organizations completed a brief demographic data form (age, gender and ethnicity) and administered the Children’s Hope Scale (Snyder et al., 1997) the day of surf therapy before departing to the beach. After returning from surf therapy (on the same day), staff from partner organizations administered the Drawing Form and the Children’s Hope Scale. Finally, the Children’s Hope Scale was administered by staff from partner organizations one-month after participating in surf therapy. Partner organizations providing ongoing mental health or foster care were able to collect one-month follow-up data on hope and additional demographic data.
Data Analysis
Using IBM SPSS Statistics 25, analyses compared mean scores on children’s hope before, after and one month after participation in ocean therapy. A paired samples t-test was conducted to analyze for statistically significant differences on children’s hope mean scores before and after participation in ocean therapy for a sample of 152 participants. For a subsample with one-month follow up data, a one-way within subjects ANOVA was conducted to analyze for statistically significant differences on children’s hope mean scores before, after and one-month after ocean therapy for a subsample of 50 participants. Two cases missing three and five responses from the follow-up hope scale were excluded from analysis resulting in a subsample of 50 instead of 52.
Results
Process evaluation. Based on the ratings of 157 drawings and related text reflecting participants’ experience of the day on four program process indicators, 92% (n=145) of participants expressed experiencing Opportunities for Learning and Fun, 77% (n=121) expressed a positive attitude about their Self-identity or Self-concept, 61% (n=95) expressed Feeling Safe, and 58% (n=91) expressed experiencing Social Support and Inclusion.
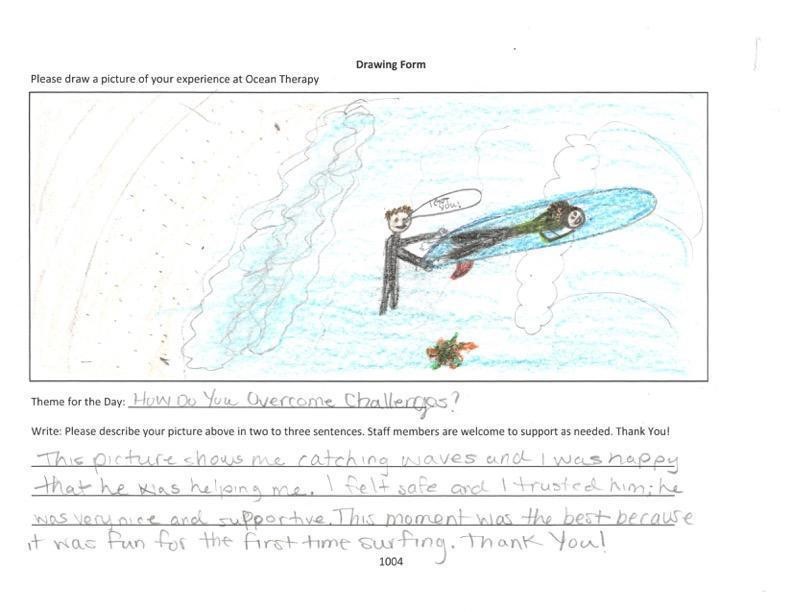
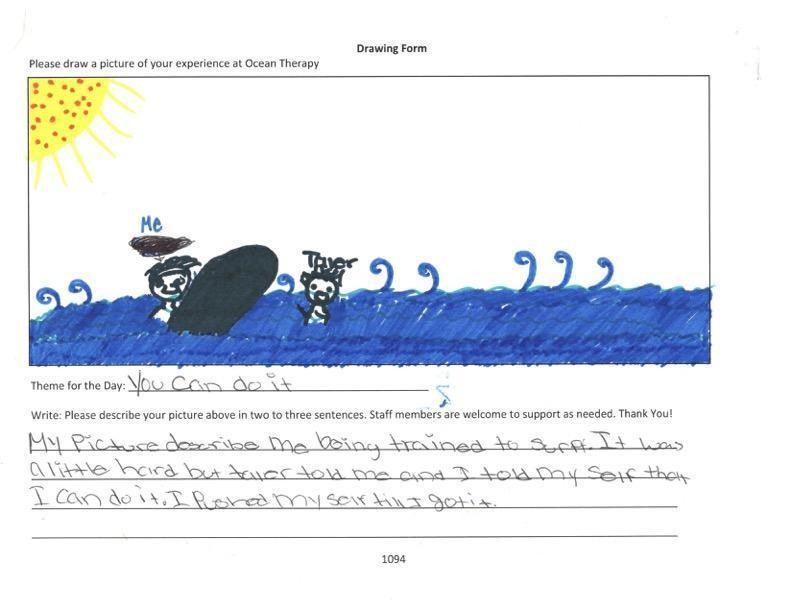
Figures 1, 2 and 3 (to see figures, download the PDF version to access the complete article, including Tables and Figures) present samples of participant drawings rated as including all four program processes described above. Additionally, demographic data indicates that each of the participants experienced adverse experiences and personal challenges. Figure 1 (to see Table 3, download the PDF version to access the complete article, including Tables and Figures) presents the drawing and associated text of a 15-year old, female participant, identifying as Hispanic or Latino, with a history of trauma, emotional or behavioral problems, child abuse or neglect and substance or alcohol use. Figure 2 (to see Table 3, download the PDF version to access the complete article, including Tables and Figures) presents the drawing and associated text of a 14-year old, female participant, identifying as African American, with a history of trauma, emotional or behavioral problems, and child abuse or neglect.
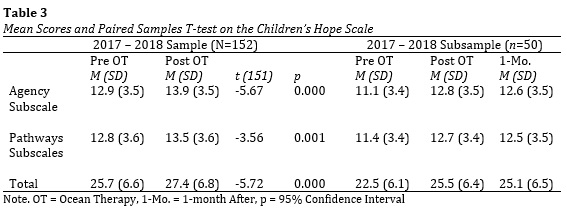
Outcome evaluation. Two data sets are presented in this section. The first includes pretest and posttest mean scores on the Children’s Hope Scale (Snyder et al., 1997) for 152 participants. The second data set is a smaller subsample (n=50) that includes pretest, posttest and one-month follow-up mean scores on the Children’s Hope Scale. Table 3 (to see Table 3, download the PDF version to access the complete article, including Tables and Figures) presents means for subscale and total scores on the Children’s Hope Scale for both groups. Results of a paired samples t-test are also included, comparing mean scores on Children’s Hope before and after participating in ocean therapy (N=152). There was a statistically significant increase in mean scores on the Children’s Hope Scale (subscale and total mean scores) between pretest and posttest.
Because the t-test was statistically significant, a one-way within-subjects ANOVA was performed to test whether there was a difference in mean total scores on Children’s Hope before ocean therapy, after ocean therapy, and one-month after ocean therapy for the subsample of 50 participants. While two of the underlying assumptions (independent observations & multivariate normal distributions) for ANOVA were met, the assumption of sphericity was violated, as indicated by Munchy’s Test of Sphericity, and the Greenhouse-Geisser corrected value was used. The observed F value was statistically significant, F(1.6,49)=11.25, p=0.000, partial n^2=.187, which indicated a positive difference in mean scores on the Children’s Hope Scale observed between pre and post-test and sustained one-month after participation.
Discussion
The main hypothesis of this study, it is hypothesized that one of the benefits to participation in a one-day surf therapy program is a significant increase in hope, was supported by a statistically significant increase in hope between pre and post-test (N=152) and sustained one month after (n=50). The subsample of participants who were primarily Latino and African-American experienced an average of 1.69 adverse experiences (i.e., trauma or child abuse or neglect) and/or personal challenges (i.e., emotional/behavioral problems, learning disability or educational difficulties, or substance/alcohol use/abuse). This subsample is representative of at-promise youth and the results are promising. Participants of the Jimmy Miller Memorial Foundation’s (JMMF) one-day ocean therapy program included in this study experienced a significant increase in hope that lasted up to one month after participation. While a statistically significant increase in hope was observed between pretest and posttest and pretest and one-month follow-up, results do not imply cause due to the observational design of the study.
Elements of the JMMF ocean therapy program include talking circles, surf instruction and lunch, all of which include interactions with peers, volunteers, surf instructors, the program director and other program/partner organization staff. Considering surf therapy programming varies greatly between programs and there are no standardized program process measures for surf therapy programs, study staff developed a method to assess program process. This method includes rating participants’ drawings and related text on their experience of the day administered immediately after returning from ocean therapy. Drawings and related text serve as participants’ visual and text depictions of their experience of the day which serve to inform JMMF program process. The coding system provides criteria for raters to assess for program process indicators through participant self-expressions in four areas - safety, social support and inclusion, learning something new and having fun, self-identity or self-concept. It is hypothesized that if participants express positive program process indicators through their drawings, they will be more likely to experience an increase in hope.
Contribution to the Literature
The current study is the first of its kind to evaluate a one-day surf therapy program for youth at-promise. Observational studies have explored one-day surf therapy programs for adult populations and youth with disabilities but not youth at-promise. The current study builds upon previous research using hope as an outcome measure for surf therapy. Only one other study (Snelling, 2015) examined hope as an outcome for surf therapy and did not find any significant differences between a control and surf therapy conditions. However, study methodologies, including a significantly longer period of time between pre- and post-tests (i.e., same day and four weeks vs. 32 weeks) and a much longer surf therapy program may explain the difference in findings. Perhaps differences in hope are more salient immediately following a session of surfing. Additionally, there were no obstacles in the collection of follow-up data for the current study whereas Snelling (2015) reported difficulties in obtaining follow-up data (35.6% drop-out rate).
Finally, the results of the current study are consistent with the findings of studies on three other programs reviewed in this paper that utilized an observational design and found statistically significant increases in one or more measures of wellbeing (e.g., increases in self-concept, emotional regulation, and social competencies) (Taylor, 2013; Colpus & Taylor, 2014; Godfrey, et al., 2015; Hignett, et al., 2017; and, Matos, et al., 2017).
Limitations of the Current Study
While the results of this observational study indicate that therapeutic benefits (i.e., increase in hope) were achieved by youth at-promise through a one-day surf therapy program, causal attribution would require an experimental design. Additionally, due to the observational design using a convenience sample, the generalizability of the results of this study to other groups is limited. And, given that three of the five partner organizations only included youth who were exhibiting prosocial behaviors, results of this study may have been skewed. Future studies on one-day surf therapy programs should consider utilizing comparison or control groups if possible. Given the limited funding for research among most surf therapy programs, utilizing non-equivalent comparison groups may be the most realistic starting point.
It is unclear as to whether results obtained were related to a certain aspect of the program (i.e., surf instruction vs. talking circles) or the complete experience of the JMMF one-day ocean therapy program. A common factor among many surf therapy programs is the effect of surfing in relation to the effect of other programming directed toward promoting participant well-being. In the current study, talking circles served as a means for sharing and community building. Talking circles were separate from the surf lessons and the roles of each alone are not well understood in their relationship to hope. A quasi-experimental design with intervention groups receiving surf lessons and talking circles or surf lessons only could address this issue.
The outcome evaluation used the Children’s Hope Scale which has been validated only with youth populations between the ages of 8 and 16, however, 5.3% (n= 8) of our sample was over the age of 16. Additionally, two cases were removed from the subsample due to missing responses from the one month follow up hope scale. And, some participants participated during both years of data collection although none participated more than once a year. Because the pretest and posttest were administered on the same day, immediately before and after surf therapy, it is less likely that maturation or history (i.e., two common threats to internal validity) impacted these results than with the one-month follow-up data. Yet, it is also more likely that data were impacted by practice effects – completing the hope scale twice in the same day.
The process evaluation utilized a self-constructed method that was informed by previous research and adapted to reflect the JMMF one-day ocean therapy program process. Through rating participant drawings on four program process indicators, raters generate numeric frequencies of unsolicited self-expression for each program process indicator. Because the process of rating requires that raters interpret drawings and text, there is an increased risk that bias could impact the rating process. To reduce this risk, an additional rater was added as a judge to resolve discrepancies in ratings and an inter-rater reliability analysis was conducted and interpreted as having a strong level of reliability among raters. Yet, there is no research evidence to support this method of process evaluation and it is likely that as long as programs include differing psychosocial interventions alongside surf lessons or surfing in surf therapy programs, a standardized process evaluation measure will be difficult to develop.
Conclusion
Results of this preliminary study suggest that surf therapy may be an effective intervention to increase hope among youth at-promise. Participants experienced a statistically significant increase in hope after participation that was sustained one-month after participation in the JMMF one-day ocean therapy program. The observational single group pretest-posttest-follow-up research design serves an important program evaluation function in supporting program effectiveness, yet, is limited in identifying causal attributes and in generalizing results to other populations and settings.
References
Armitano C., Clapham, E.D., Lamont, L. & Audette, J. (2015). Benefits of Surfing for Children with Disabilities: A Pilot Study. Palaestra, 29.
Assembly Bill No. 413, CA Education Code, Section 96 (2019). Retrieved from https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201920200AB413.
Benninger, E. & Savahl, S. (2016). The Children’s Delphi: Considerations for developing a programme for promoting children’s self-concept and well-being. Children’s Delphi programme considerations. Child and Family Social Work, 22(2), 1094-1103. doi: 10.1111/cfs.12329.
Britton, E., Kiindermann, G., Domegan, C., & Carlin, C. (2018). Blue care: A systematic review of blue space interventions for health and wellbeing. Health Promotion International, 1-20. DOI: 10.1093/heapro/day103.
Caddick, N., Smith, B. & Phoenix, C. (2015b) The effects of surfing and the natural environment on the well-being of combat veterans. Qualitative Health Research, 25, 76–86.
Carin-Levy, G., & Jones, D. (2007). Psychosocial aspects of scuba diving for people with physical disabilities: an occupational science perspective. Canadian Journal of Occupational Therapy, 74, 6-14.
Casey, N., O’Broin, D., & Collins, B. (2009). The meaning of the experience of kayaking for persons with spinal cord injury. Irish Journal of Occupational Therapy, 37, 29-36.
Clapham, E.D., Armitano, C.N., Lamont, L.S. & Audette, J.G. (2014). The Ocean as a Unique Therapeutic Environment: Developing a Surfing Program. Journal of Physical Education, Recreation & Dance 85, 8-14.
Colpus, S. & Taylor, J. (2014). Ride every challenge: the impact of surfing on 100 young people facing personal and emotional challenges. British Journal of Sports Medicine, 48, 1581. doi: 10.1080/07303084.2014.884424.
Court Appointed Special Advocates (CASA). (2015). L.A.’s 30,000 children in the foster care system need our help! Retrieved from http://www.casala.org/wp-content/uploads/2015/04/CASA-Fact-Sheet.pdf
Czikszentmihalyi, M. (1990). Flow: The psychology of optimal experience. Harper Collins Publisers. New York, NY.
Dustin, D., Briker, N., Arave, J., Wall, W., & West, G. (2011). The promise of river running as a therapeutic medium for veterans coping with post-traumatic stress disorder. Therapeutic Recreation Journal, 45, 326.
Farley, O.R., Harris, N.K., & Kilding, A.E. (2012). Physiological demands of competitive surfing. Journal of Strength Conditioning Research, 26(7), 1887-96.
Felitti, V. J., Anda, R.F., Nordenberg, D., Williamson, D.F., Spitz, A.M., Edowards, V., Koss, M.P., & Marks, J.S. (1998). Relationship of child abuse and household dsyfunction to many of the leading causes of death in aduilts. The Adverse childhood experiences (ACE) study. American Journal of Preventative Medicine, 14(4), 245-58.
Gilman, R., Dooley, J., & Florell, D. (2006). Relative levels of hope and their relationship with academic and psychological indicators among adolescents. Journal of Social and Clinical Psychology, 25(2), 166-178. doi: 10.1521/jscp.2006.25.2.166.
Godfrey, C., Devine-Wright, H. & Taylor, J. (2015). The positive impact of structured surfing courses on the wellbeing of vulnerable young people. Community Practice (88) 26-29.
Hignett, A., White, M.P., Pahl, S., Jenkin, R. & Froy, M.L., (2017). Evaluation of a surfing programme designed to increase personal well-being and connectedness to the natural environment among ‘at risk’ young people. Journal of Adventure Education and Outdoor Learning, 18(1), 53-69. doi: 10.1080/14729679.2017.1326829
Los Angeles County Department of Mental Health (LACDMH). (2017, July). Quality improvement work plan evaluation report 2016 and quality improvement work plan 2017. Retrieved from Los Angeles County Department of Mental Health website: http://file.lacounty.gov/sdsinter/dmh/1029995_QIEVALREPORTCY2016.pdf
Los Angeles County Department of Public Health (LACDPH). (2011, September). Obesity and related mortality in Los Angeles county. Office of Health Assessment and Epidemiology, Los Angeles County Department of Public Health.
Martinek, T.J. & Hellison, D.R. (1997). Fostering resiliency in underserved youth through physical activity. Quest, 49 (1), 34-49.
Matos, M.G., Santos, A., Fauvelet, C., Marta, F., Evangelista, E.S., Ferreira, J., Moita, M., Conibear, T., & Mattila, M. (2017). Surfing for social integration: Mental health and well-being promotion through surf therapy among institutionalized young people. Journal of Community Med Public Health Care, 4 (26), 1-6. doi: 10.24966/CMPH-1978/100026.
Moore, A.M., Clapham, E.D. & Deeney, T.A. (2018). Parents’ Perspectives on Surf Therapy for Children with Disabilities. International Journal of Disability, Development and Education, 65(3), 304-317. doi: 10.1080/1034912X.2017.1400660
Morgan, P. (2010). Get up. Stand up. Riding to resilience on a surfboard. Child and Family Social Work, 15, 56-65. doi: 10.1111/j.1365-2206.2009.00637.x.
Mueller, M. (2017). Surf therapy for students with ASD (Unpublished doctoral dissertation). California State University, San Marcos.
Piaget, J. (1964). Cognitive development in children. Journal of Research in Science Teaching, 2, 176-186.
Pittsinger, R., Kress, J., & Crussermeyer, J. (2017). The effect of a single bout of surfing on exercise-induced affect (unpublished master’s thesis). Department of Kinesiology, California State University, Long Beach, CA, USA.
Rogers, C.M., Mallinson, T., & Peppers, D. (2014). High-intensity sports for posttraumatic stress disorder and depression: feasibility study of ocean therapy with veterans of Operation Enduring Freedom and Operation Iraqi Freedom. American Journal of Occupational Therapy, 68, 395-404.
Sharabi, A., Levi, U. & Margalit, M. (2012). Children’s loneliness, sense of coherence, family climate, and hope: Developmental risk and protective factors. The Journal of Psychology: Interdisciplinary and Applied, 146, (1-2), 146. DOI: 10.1080/0223980.2011.568987.
Snelling, M. (2015). Breaking cycles of violence, one wave at a time: A formative evaluation of the waves for change surf therapy programme (master's thesis). University of Cape Town, Cape Town South Africa.
Snyder, C. R., Hoza, B., Pelham, W.E., Rapoff, M., Ware, L., Danovsky, M., Highberger, L., Rubinstein, H., & Stahl, K.J. (1997). The development and validation of the children’s hope scale. Journal of Pediatric Psychology, 22(3), 399-421.
Taylor, J. (2013). Giving kids a break: How surfing has helped young people in Cornwall overcome mental health and social difficulties. Mental Health and Social Inclusion, 17(2), 82-86. doi: 10.1108/20428301311330135.
Valle, M.F., Huebner, E.S., & Suldo, S.M. (2006). An analysis of hope as a psychological strength. Journal of School Psychology, 44(5), 393-406. doi: 10.1016/j.jsp.2006.03.005.
Wheaton, B., Roy, G. & Olive, R. (2017). Exploring Critical Alternatives for Youth Development through Lifestyle Sport: Surfing and Community Development in Aotearoa/New Zealand. Sustainability, 9, 2298.
Wolstein, J., Babey, S.H., & Diamant, A. L. (2015, June). Obesity in California. Los Angeles, CA: UCLA Center for Health Policy Research. doi: 10.1016/j.healthplace.2017.04.010.
 Gregor V. Sarkisian, Chloe Curtis, & Carly M. Rogers
Gregor V. Sarkisian, Chloe Curtis, & Carly M. Rogers
Gregor V. Sarkisian, Professor, has taught in the Applied Community Psychology specialization within the M.A. in clinical psychology program at Antioch University Los Angeles since 2005.
Chloe Curtis, Research & Evaluation Team Coordinator for the Jimmy Miller Memorial Foundation. She earned her BA in Marketing, and MA in Education from Loyola Marymount University. She is now working on her second masters in Counseling at Loyola Marymount, while coaching the Division I men’s and women’s Cross Country and Track teams.
Carly M. Rogers, clinical occupational therapist and independent researcher. She received her BA in Psychology from the University of California at Santa Barbara and her masters and clinical doctorate in Occupational Therapy from the University of Southern California.
agregar comentario
![]() Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
palabras clave: surf therapy, youth at-promise, one-day surf therapy program
 Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.
Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.