



Worldwide, obesity is a growing epidemic and a leading non-communicative disease. Egypt has high levels of obesity, which is causing harm to both individuals and society. This study aimed to collect data on available programs and interventions, to assess gaps and explore assets and challenges to obesity programming in Egypt. The purpose of this article is to examine obesity from an ecological perspective, direct practical work related to obesity to help fill these gaps. Semi-structured interviews were conducted with 25 participants from 22 different organizations, including ministries, governmental, non-governmental, international organizations, and for-profit organizations. Finally, participants provided their personal recommendations for combating obesity in Egypt. The findings from this research showed that there is a lack of nationwide programs and services that tackle obesity; however, there are some minor activities and services that tackle other health issues related to obesity. This information is beneficial to connect programs and build coalitions. Participants related their challenges to mainly contextual and ecological factors and recommended collaboration, partnerships and multi-sectorial programs on a mass scale including national campaigns to get obesity recognized and on the national agenda. Recommendations can help develop prevention strategies that are tailored to the socio-cultural and economic context of Egypt and similar countries.
Download the PDF version to access the complete article, including Tables and Figures.
Obesity definition, consequences, and prevalence
Obesity is a condition of excess body fat (Ravussin & Swinburn, 1992); an imbalance between calories consumed and calories burned (Zulet, Berkenpas & Martinez, 2005). Obesity and overweight are usually mentioned together, as obesity is an advanced stage overweight. Defined by the National Institute of Health (NIH) as a Body Mass Index (BMI) equal to or above 30. Early-onset obesity may lead to physical and psychological co-morbidities, while it contributes to non-communicable diseases (NCDs) such as type-2 diabetes, cardiovascular diseases, and some types of cancers (Summerbell et al., 2005; WHO, 1997). Obesity is linked to some mental health problems, such as eating disorders and low self-esteem (Seo & Sa, 2010). Obese children and adolescents are prone to physical health problems (Agency for Healthcare Research and Quality (AHRQ), 2013), as well as have a greater chance of becoming overweight or obese adults (Georgetown University Center for Aging, 2002; Lawlor, Smith, & O’Callaghan, 2007; Singh, Mulder, Twisk, Van Mechelen, & Chinapaw, 2008). No matter the stage of development, obesity both affects the quality of people’s lives and may also shorten their lives (Sturm, 2002). More so, the stigma regarding weight is both societal and self-imposed (Major, Eliezer & Rieck, 2012); and becomes a physical and psychological threat to a person’s health. Also, stress contributes to overweight and obesity, as well as being a consequence of obesity and overweight (Becton, Shatat, & Flynn, 2012; Pervanidou & Chrousos, 2011). Conclusively, obesity burdens countries’ health systems with direct and indirect costs (Colditz, 1992; Withrow & Alter 2010).
Worldwide, obesity is growing, it is considered an epidemic and a leading non-communicative disease (Alpert, 2009; International Association for the Study of Obesity [IASO], 2010; Kime, 2008; Owen, Martin, Whincup, Smith, & Cook, 2005; Summerbell, Waters, Edmunds, Kelly, Brown, & Campbell, 2005; World Health Organization [WHO], 2000). The percentages of obesity rose from 5% to 10% for men and from 8% to 14% for women between 1980 and 2008; and affects approximately 20-50% of children and teenagers (Cosoveanu & Bulucea, 2011). That is concerning because overweight and obesity are linked with more deaths worldwide than being underweight (WHO, 2009), and are rated as the fifth leading risk for global deaths (WHO, 2008).
Obesity is highly prevalent in Egypt (Asfaw, 2006; Atinmo, Mirmiran, Oyewole, Belahsen, & Serra-Majem, 2009; Ellabany & Abdel Nasser, 2006). The estimated prevalence of overweight and obesity (BMI ? 25 kg/m²) is 61-70% of the whole population aged 20 and above. Research indicated that 65% of males and 76% of females aged 15 and above to be overweight and obese. As for obesity alone, 18-22% of males are obese while 39-48% of females are obese (Ellabany, & Abdel Nasser, 2006; IASO, 2012; WHO, 2010). Also, obesity is one of the top contributors to the national mortality and morbidity of Egyptians along with other noncommunicative diseases (NCDs). Chronic NCDs cause 41% of all mortality in Egypt (FAO, 2006). NCDs are reported to be the main cause of morbidity and mortality in Eastern Mediterranean Countries and are emerging as a major health problem in Egypt. This is alarming and calls for action, not only in Egypt but in neighboring countries and worldwide. Alas, research in Egypt has been focusing on the prevalence of obesity and not on causes or solutions. Yet, it is important to move away from victim-blaming and target the issue from an ecological perspective.
Using the ecological framework by Prilleltensky, Nelson, and Peirson, (2001)adopted from the ecological systems developed by Bronfenbrenner (1977), we can look at the issue from a more holistic perspective. The ecological framework suggests that a person does not exist alone but is a part of a community and society and that as researchers design interventions we must understand and accordingly make changes that would reach the individual through their micro, meso, exo and macrosystems in which they live. The microsystem consists of the direct structure around a person’s life for example, their family, neighborhood, and school. This is where the person’s eating habits are established, and nutrition education classes are related to obesity could be beneficial. The macrosystem relates to the culture, media influences, policies of the country that influence the behaviors of the individual. An example would be creating policies to change the fat content in school lunches or increase physical activity in the school curricula to address obesity in Egypt. The systems between micro and macrosystem are the mesosystem and exosystem, these relate to the linkages between systems. The exosystem relates to an individual’s microsystem and another setting such as local government and the school lunch program or grocery store’s program to purchase healthy snacks. The mesosystem targets the connection between all the layers between an individual’s unhealthy or sedentary lifestyle and the school system and between local resources in the community.
Obesity in an Ecological Framework
Although research on obesity in Egypt is mainly focused on the prevalence of obesity, the following section will explain the factors that contribute to obesity. To adequately address the issues faced in Egypt regarding obesity, an ecological framework will guide this research on the following dimensions: The individual, the microsystem (school and family) and the macrosystem (society and culture). Obesity on the individual system focuses on biological and physiological characteristics. However, although there are biological influences on a person’s weight (Farooqi, 2006; Hu, 2008), genetics alone cannot explain the growing epidemic of obesity worldwide (Hu, 2008; Veerman, 2011). Furthermore, other individual factors contribute to a person’s state of obese. These factors include nutrition and physical activity, changes in lifestyle, and activity level– the fundamental principle of the energy balance equation (WHO, 2000) –as well as level of education. The more educated the lower the probability of obesity (Devaux, Sassi, Church, Cecchini, & Borgonovi, 2011). Supposedly, education provides more knowledge and greater access to health-related information, which motivate and improve self-control (Devaux et al., 2011). Yet, it is still prevalent among the educated and wealthy in Egypt; 40.9% of wealthy higher educated women and 53.9% of wealthy uneducated women (Aitsi-Selmi et al, 2012).
A microsystem level of an individual shows that family plays are role in obesity as the major contributor to most habits related to eating (Epstein, 1996). Egypt being a collectivistic society and family being a major contributor, the effect of family is great on obesity. Obese parents tend to over nourish their children (Sobko, Svensson, Ek, Ekstedt, Karlsson, Johansson, Cao, Hagströmer, & Marcus, 2011). In 2000 around 47% of Children in Egypt received more than 100% of their Recommended Daily Allowance (RDA) compared to 14% in 1995 (FAO, 2005; Hassan, Moussa, & Ismail, 2005). Additionally, family stressors, like the lack of mental and physical stimulation and financial constraints, lead to biological effects or negative health habits (Garasky, Stewart, Gundersen, Lohman, & Eisenmann, 2009). Appropriately, the family can adjust and alter the home environment and lifestyle to mitigate obesity (Golan & Crow, 2004).
As for school and university, children consume between 19 to 50 percent of their daily calories at school (Gleason & Suitor, 2001), and the availability of foods and beverages high in sugar adds to the high-calorie consumption of the students (Frumkin, 2006). Likewise, university students may experience some changes during their first year of college including weight gain due to the transition (Hajhosseini, Holmes, Mohamadi, Goudarzi, McProud, & Hollenbeck, 2006; Hudd, Dumiao, Erdmann-Sager, Murray, Phan, Nicholas, & Yokozuka, 2000; Racette, Deusinger, Strube, Highstein, & Deusinger, 2005).
On the macrosystem level, there are multiple socio-environmental factors like food subsidy and availability that affect obesity in Egypt (FAO, 2006; Traill, 2006; Larson, Story, & Nelson, 2009). There is a significant relationship between the subsidized balady (pita) bread and the BMI of Egyptian women (Asfaw, 2007); the lower the price due to subsidy, the higher the BMI. Modernization and globalization have also led to dietary changes as a result of the emergence of fast food and energy-dense foods in Egypt and the surrounding countries (FAO, 2006; Traill, 2006; Larson, et al., 2009). Factors contributing to obesity in Egypt are similar, if not the same, like other countries. Most impactful is urbanization; which translated into the sedentary nature of jobs, the rise in “energy-saving” devices, the speed and convenience of driving rather than walking or biking (Traill, 2006; WHO, 2003). The cultural context also plays a role in obesity, whether that being obese was an indicator of wealth exhibited around the waist (Renzaho, 2004) or ‘plumpness’ being as a sign of beauty and larger-sized women were generally accepted in Egypt (Jackson, Rashed, & Saad-Eldin, 2003). Contradictory, media has a role in feeding the misconceptions about thinness by portraying women with unattainable sizes for the normal population as the symbol of beauty and desirability (Cohen et al. 2005). Yet, it is also important to note that media reinforce the stigma of obesity by their popular advertisements showing how weight is all about personal control (Geier, Schwartz, & Brownell, 2003). Excess consumption of food or discouraging physical activity is also incorporated in the media, which affects people’s weight gain (Glanz, Sallis, Saelens, & Frank, 2005; Glanz, Sallis, Saelens, & Frank, 2007; Grier and Kumanyika, 2008).
All these factors on the different ecological levels contribute to obesity and accordingly, interventions need to target all levels and systems. Consequently, organizations on different levels and in all sectors should be involved in efforts regarding obesity. To know how much a country is working on an issue, it is important to see how its organizations are contributing to solving the issue. Not only the efforts of the government or policy changes and the public sector efforts, but also efforts of organizations of the private, for-profit, and non-profit sectors.
The Study
The aim of the study was to identify gaps and assets of obesity interventions in Egypt. This was done through mapping available programs and interventions and collecting information about activities, interventions, or programs done in the past five years, were ongoing or were planned for the next five years. Ultimately to explore best practices and challenges to obesity programming and provide recommendations for practice. Based on the current literature, the main broad research questions were: (1) What factors, such as assets and resources, contribute to the availability of obesity programs, initiatives, and policies in Egypt? (2) What are the challenges faced when providing obesity-related programs, initiatives, and policies?
Methods
Participants
Semi-structured interviews were conducted with 25 staff working in or who are members of 22 organizations from the private/for-profit, public, and nonprofit sectors. In three organizations, interviews were conducted with more than one official, and three participants covered the work of two different organizations each. Organizations were chosen based on their potential relevance to obesity and participants were asked about their activities in all Egyptian governorates.
The participants provided information about 10 for-profit organizations; a pharmaceutical company, a fast-food chain, a food production company, an individual initiative providing diet foods, a physical education private academy, a chain of gyms, private sports and fitness therapy centers, fitness programs and physical activity initiatives, and a sport promotion services company. Seven civil society organizations were a part of the study; three Egyptian organizations, two United Nations Agencies, and two international organizations. Five national governmental organizations; the Ministry of Health, the Ministry of Youth and Sports and its subordinate organizations, the National Research Center, an Egyptian university of physical education, and the National Nutrition Institute.
Recruitment of participants
A list of major organizations was put together to include organizations from the public, private and non-profit sectors. Participants from an initial list were contacted and others were further interviewed based on the snowball sampling approach. Through personal connections members who are a part of these organizations were contacted. Initially, the plan was to conduct 15 interviews but due to personal connections and participants willing to help out, 25 participants were recruited. These participants were contacted through a phone call or e-mail followed by a phone call. In one case, a participant personally connected the researcher with another participant to give more information about the work the organization was doing. All initial participants who were contacted responded because they have been referred through a common contact, and social relationships are very important in Egypt. Knowing that the researcher was contacting them based on someone’s referral higher the chances of getting responses from participants. As the study is exploratory, and the list of potential organizations was preset, the researcher tried to reach respondents in these organizations through social connections and not simply send out emails and wait for the response. All participants contacted were reached and interviewed.
Interview procedure
One pilot interview with a key informant was conducted followed by 25 interviews of 22 organizations at the participants’ offices, and three interviews by phone. The interviews lasted from 15 minutes to a little over an hour. Participants answered in English and/or Arabic, mostly a mixture of both. Accordingly, direct quotes are difficult to publish. The semi-structured interview responses were audio-recorded with participant approval, table1 illustrates interview questions (to see Table 1, download the PDF version to access the complete article, including Tables and Figures). A data collection sheet was used to record the answers to the interview, as well.
Measures
Interview questions were developed based on the literature review. They were designed to elicit assets and challenged and a database of the prevention and intervention programs in Egypt relating to obesity. This information aims to highlight the gaps in the services and programs on ecological levels and geographically. Interviews were composed of eight main questions with follow up questions.
Data Analysis
All interviews were transcribed from recordings or notes. A thematic analysis was conducted, and the themes were extracted for each question and a codebook was created. Data were organized under the questions and then divided by codes. Each code/category was examined to determine consistency among the text within the code, and codes were adjusted when necessary (De Negri & Thomas, 2003). The initial codebook was composed of ‘middle-order’ categories (Dey, 1993), meaning that the codes were further developed to include more details as the process went on. The final codebook was created through merging similar codes or the alteration of some codes. Data was sent to a fellow community psychology researcher to test for inter-rater reliability. Consistency was shown between raters and there were no discrepancies.
Results
The results of the study include information about the interventions and programs implemented by the different organizations and individuals that were interviewed. The data included obesity-specific interventions as well as related efforts such as nutrition education or wellness initiatives. After analysis, the data collected was organized by age of target audience, geographical location, and gender; according to their ecological levels to identify the gaps in service. The information was organized by intervention, scope, timing and duration, and target audience. Specific data of the programs by the different organizations are published in a thesis (Shahin, 2015). For the purpose of this paper, it is important to note that most organizations did not target obesity directly and only 11 organizations had set plans; like the national multi-disciplinary nutritional strategy. Most initiatives did not have reducing obesity as one of its goals. Further gaps that were identified are the location and availability of the interventions; such as being centralized in the larger governorates and not accessible to everyone. Interventions were mainly in Cairo and Alexandria, or through governmental health clinics that may reach some smaller governorates. Furthermore, interventions were more targeting females than males.
Focusing on challenges and assets, the main and subthemes are presented in the table below. The themes were these broad themes across all organizations interviewed. While the data of the interventions were specific to the Egyptian setting, the challenges, and assets, however, are more generalizable to different settings and areas, and can be seen as complementary in many cases. Table 2 (to see Table 2, downlad the PDF vesion to access the complete article, including Tables and Figures) demonstrates the different subthemes and exemplars of these subthemes that are under the two main theses; challenges and assets. Most challenges are on the macro, meso and exo systems; cultural habits and misconceptions, lack of awareness and education about nutrition and health, the political situation in Egypt, environmental factors, facilities, and infrastructure and financial expenses and funding. Mostly, the Egyptian culture and societal habits, in addition to misconceptions about nutrition and exercise, were viewed as the main contributors to obesity and to the low number of activities and services provided to combat it. These misconceptions include viewing fatness as a sign of wealth and incorrect information about nutrition and health practices. Also, unhealthy cooking techniques, such as overcooking vegetables so that they lose their vitamins or overconsumption of carbohydrates. Additionally, participants explained that there is a misconception that being healthy and having a nutritious diet is perceived as a luxury or means to lose weight and not a lifestyle. Furthermore, the lack of physical literacy is related to low engagement in physical activity. Gender roles also contributed to low physical activity, as one participant said: “women thinking that they should not lift weights or they would look manly, [and] men who think aerobics is just for women; cultural misconception of fitness in general.” Also, modernization and the sedentary lifestyles adopted by the general population was mentioned. modernization was explained as the use of energy-saving devices, cars, and elevators. Also, working mothers who cannot breastfeed for the entire first six months because they must go back to work deprive infants of proper nutrition and adds to the epidemic. Program-specific challenges are least mentioned and would fall in the microsystem.
Participants were also asked about resources or assets that they think can benefit obesity interventions and how can they be obtained. Here are their recommendation; nutrition education (n = 17), policy and governmental action (n = 16), multi-sectorial programs and partnerships (n = 11), media as a channel of communication (n = 11), physical activities and sports practices (n = 10), health and sports education (n = 10), facilities and infrastructure (n = 6), funding and budget allocation (n=4).
Discussion
The data showed that there is a lack of focus on obesity; which may be related to the continuation of the spread of the epidemic. Organizing the interventions based on purpose, ecological levels and geographical location, highlighted the lack of adequate obesity interventions in Egypt. Gaps are showing that obesity is not on governmental agendas and the political situation is causing harm to the interventions. Most programs and strategies, as stated in Egyptian literature, are geared towards malnutrition rather than obesity, because the focus is mostly on stunting and malnutrition, while under-nutrition is no longer the major concern (FAO, 2006). Also, current efforts are inadequate for addressing the problem. Participants stated that there is a lack of nationwide programs, initiatives, and campaigns; in addition to the lack of knowledge and awareness of the public related to obesity interventions. Most interventions are in major governorates.
Outreach and availability
Almost all programs and services are available to both men and women with more focus on females yet does not guarantee that they are successful or reach the females because of cultural barriers and norms. Accordingly, the gaps are not the only reason for the inefficiency of programs but there are other challenges that need to be addressed. These challenges include cultural misconceptions and barriers, that can be overcome by awareness spreading. Another challenge is poverty and food safety; which need a more collective approach that is multilayered. Policy can also help with overcoming infrastructural challenges and controlling the media to stop feeding the misconceptions about thinness and reinforce the stigma of obesity and promoting unhealthy foods and eating habits. Also, implementing the policies is necessary to decrease the violation of policies controlling food products.
Location and availability of interventions
Addressing the location of the interventions is important because it can show how distributed they are. Most programs were in major cities and so do not meet the greater need all over the country; still, minimal outreach to the rest of the country is through governmental programs. Although they do not target obesity directly, these outlets and great outreach can be utilized in the fast dissemination of future programs. The map only demonstrates potential outreach of programs and services (figure 1;to see Figure 1, download the PDF version to acces the complete article, including Tables and Figures) but not the actual impact of these activities and can be used to further plan distribution and outreach strategies for new programs or activities.
The biggest challenges that participants have mentioned were the cultural habits and misconceptions. These include unhealthy lifestyles and habits that encourage high levels of calorie intake. Also, modernization and sedentary lifestyle have contributed to the Egyptian society’s activity levels, negatively. That in addition to the lack of culture of sports and the lack of awareness and education about nutrition and health. Participants believe that people are unaware of healthy choices and practice and neglect their general health; which makes it harder for the interventions to be effective and have people stick to them.
Additionally, since the revolution in 2011, the political situation in Egypt has been putting some strains of non-profit funding; which has affected some programs. Also, some safety concerns and changes in the government ever since has added to a general atmosphere that destructed some plans.
Service and program-specific challenges
Furthermore, interventions and services, as well as being stated by participants, are fragmented or targeting factors of obesity, without a holistic view. There is a need for programs to be multi-faceted interventions. Furthermore, many are targeting the individual and do not look at obesity from a multi-systems approach. Accordingly, and based on literature, strategies need to be geared towards the family, the community and the government. Also, stakeholders and the targeted population should be included in planning and creating healthy environments. Children’s activities provided are not enough to prevent obesity as they are not combined with home or community, services to the family as a whole prove to be most effective (Campbell Sahin-Hodoglugil, & Potts, 2006). Furthermore, school canteens and snacks in the neighborhoods are adding to the children’s malnutrition and can lead to obesity (Hadley et al., 2010); and school snack provided in government schools is not enough to deal with malnutrition. Accordingly, policy changes that affect school canteens and school lunches are needed in Egypt. Also, the focus on the individual may foster stigma and prejudice against obese and overweight people as having poor health and character. Teasing about weight is associated with low self-esteem and suicidal thoughts and attempts, while the emotional factors that come with obesity were not targeted in any of the programs and services.
Also, services and programs in Egypt are not on the macrosystem level and have not become national movements or achieved public consensus. They are mainly about fortifying certain foods that deal with malnutrition and benefit a certain segment of the population. These fortified foods are likely to contribute to obesity. Yet, the newly introduced national surveillance system has the potential to be a great asset. Unfortunately, research suggests that the benefit of surveillance is still debatable (Folta et al, 2006), and its potential hazards have not yet been fully studied. There is a lack of interventions that worked on the meso or exosystem levels. Yet give room for improvement and collaboration between and within the different systems provide healthier nutritious diets are possible.
Additionally, societal issues like poverty, physical infrastructure, different sub-cultures, and availability and access to foods are not considered. Most remarkably, generalizability, quality, and consistency of programs are jeopardized due to the lack of resources to expand. This calls for collaboration and collective impact initiative as none of the programs or initiatives work on multiple ecological levels. The community context should be essential to obesity prevention since there are risk factors related to eating and activity levels which affect the larger population. Nonetheless, adding a community activity component helps the effectiveness and reach of programs (Huhman & Patnode, 2013).
Assets
Participants have mentioned many assets that can be utilized to counter challenges and also fill the gaps. Human resources and manpower were mentioned in challenges as well as assets. There is a need for proper training and supervision to be able to capitalize on such assets and benefit from human power in implementing programs and spreading awareness. Media and social media were also mentioned as challenges but also as a major asset and channel of communication; a great way to reach out and spread information, including social media. Research, although unused many times, and research outcomes were considered an asset. Most interestingly, participants mentioned partners and networks as a potential asset, especially with different organizations on multiple levels. Supporting partnerships and networks are evident for the benefit of collaborations.
These assets have been explained as what kept the interventions going. Yet, for these interventions to spread and to enhance their effectiveness, participants agreed that obesity needs to be put on Egypt’s agenda. This would encourage cooperation between different sectors. These assets require a strong network and cooperation among different organizations to magnify the effect of the services provided. Also, spreading awareness to the general public and changing misconceptions about nutrition and exercise are essential to enhance the effectiveness of the programs. If the assets of the different organizations, be it their human resources, partners, services or reputation, are combined and enriched through collaborations and partnerships, the would help in combating obesity. Outreach and macrolevel initiatives seemed to be the major challenges, yet the organization saw that their services and people are an asset. Accordingly, getting the different organizations to cooperate and including the government and its networks, would help overcome these challenges.
Recommendations
Individual-level interventions. Research recommendations align with the findings and participants’ recommendations. In Egypt, research about malnutrition, anemia, and stunting is more prevalent. Obesity research and interventions are needed in Egypt and need to be on all ecological levels. As mentioned, macro-level factors have been the most commonly mentioned challenges, and accordingly, the focus should be on this level. Interventions and programs should be context sensitized and adapted to the Egyptian culture and it is very crucial to identify the factors contributing to obesity (Salazar-Martinez et al., 2005). Cultural and normative views of healthy weight and thinness need to be addressed to protect people from eating disorders (Cohen et al., 2005). The focus needs to be on obesity as a public health problem and not just a problem of individual health (Atinmo et al., 2009). Thus, the findings of the study recommended interventions that moved beyond an individual level intervention and focused more on the micro and macro systems approach.
Micro-systems interventions. Participants restated the need to spread awareness of obesity to develop a healthy culture. Inserting some changes in the culture and promoting healthy living should encourage more people to commit to and benefit from the services. This corresponded with research and recommended programs to be culturally sensitive to be able to adapt to the norms of the community and their view of a healthy body. Furthermore, the formation of safe environments in the microsystem is needed to reduce stigma. Also, an inclusive social ecological approach needs to be adapted to prevent people from using fashionable weight-loss diets (Cohen et al., 2005). Interventions need to be more health-centered and focus on shifting towards healthy behaviors to improve overall health and well-being (Bacon, Klein, Van Loan, Derricote, Gale, Kazaks & Stern, 2002). The focus should be on self-acceptance and a healthy lifestyle (Bacon, et al., 2002). Likewise, participants, as well as previous literature, recommend the direction of the focus to be put on health education. Nutrition education is recommended to change and control obesity, and promote sustainable healthy life changes (Asfaw, 2006; Atinmo et al., 2009; IASO, 2010; Traill, 2006).
Additionally, education through media, where the media encourages healthy food, active lifestyles and discourage sedentary lifestyles and unhealthy eating habits (The National Academy of Science, 2013). Services need to start in the schools and with children and mothers. School canteens and school lunches need to be modified (Hadley et al., 2010) through policy changes. Services should be provided to the family are the most efficient (Campbell et al., 2006). Universities are a potential venue for implementing health and wellness programs to encourage physical activity and a healthy lifestyle, promoting obesity prevention (Ferrara, 2009). Promoting healthy foods and encouraging physical activities should be incorporated in addition to health education (The National Academy of Science, 2013). Programs should implement a therapy/counseling component (Hadley, et al., 2010) to be able to target the different needs of the individual and promote physical and mental wellbeing.
Macro-level interventions. Again, participants’ recommendations and literature encourage taking a systems-level change approach, incorporating multiple stakeholders and addressing needs on multiple levels (National Academy for Science, 2013). These recommendations support multi-sectorial programs to be executed on a mass scale including national campaigns; a collaboration between governmental, nonprofit and the private sectors (HSC Foundation, 2009). Additionally, efforts should have centralized leadership for coordinating the planning, implementation, and evaluation of obesity prevention efforts across the country (National Academy for Science, 2013). Some stated that the government should take a centralized role in developing comprehensive multi-departmental initiatives and obesity programs; especially obesity prevention programs targeting children. Additionally, communities need to be incorporated into health promotion and obesity prevention.
Relatedly, relevant policies need to be incorporated on the national strategy level and obesity needs to be on the government’s agenda (HSC Foundation, 2009). A policy monitoring system is also needed to ensure policy-making processes and content and provide data to examine progress in obesity-related policy-making (National Academy of Science, 2013). The creation of sports facilities and infrastructure to promote physical activity, such as bicycle lanes, was also recommended by participants as part of the governmental initiatives.
To conclude, participants and literature recommend interventions and programs to be implemented on multiple ecological levels and include multi-sectoral stakeholders from all sectors and the community. These interventions need to be focusing on changing cultural misconceptions and behaviors through education and changes in the infrastructure, as well as policy changes and community efforts. Most importantly, the interventions need to be collaborative, community-based and culturally adapted to Egyptian society.
Limitations and further research
Although the study included more participants than anticipated, the small sample size can be considered as one of its limitations. Besides, the target group was composed of only high officials and the top leaders of the organization may have been a further limitation, since they may be far away from the details and on the ground implementations of the programs. Another limitation would be that all interviews were conducted in greater Cairo. Moreover, generalizability is limited due to the nature of qualitative research (Gobo, 2003). Qualitative research was needed due to the scarcity of the information regarding data on obesity interventions in Egypt and was essential to build rapport with the targeted organizations. Conducting interviews and building personal relationships was beneficial to the cultural context of Egypt, however, due to the specific nature of the research topic, it was limited. Lastly, it is not clear if the saturation of all key stakeholders in Egypt was reached and more research is needed to include more stakeholders.
Further research can improve on the limitation by including more organizations and also asking the public about their awareness of the issue, the needs, and assets. A study on the general population is beneficial to assess the cultural misconceptions that seem to be the major challenges stated. Additionally, assessments of the general level of awareness and education related to health and wellness are needed. A study that encompasses a larger pool of participants from all governorates of Egypt is needed to be able to provide more information about interventions all over Egypt. The diversity of the participants’ roles and positions in the organization is also needed to get into the intricacies of the activities, challenges, and assets. Furthermore, evaluations of the existing interventions and programs are needed to be able to improve on them and assess further needs. Devotion to research and respect for research recommendations needs to be further developed in Egypt. Research is needed to identify the individual and environmental causes of weight gain and poor nutrition (Hadley, et al., 2010). Research on the interventions and combination of interventions that are successful needs to be inventoried.
Implications
The data collected can be used to benefit the field of obesity, can be built on, and most importantly calls for more research and attention to the cause of obesity as a growing epidemic. The assessment of program assets, challenges, and what they can offer is of value to new initiatives. The recommendations of the participants and the study should be useful to the organizations interviewed and others dealing with obesity and overweight. Yet, they opened up more room for questions and research in the field of obesity than they have answered.
Although services and programs collected may not be directly targeting obesity, they may be directing small changes on the ecological levels around the issue that may positively affect it. The limited findings on obesity interventions call for further interventions and initiatives in the field in addition to further research. Further research; especially impact analysis and evaluations of the programs, to fully understand the challenges and assets, is needed.
Conclusion
Obesity has become an alarming epidemic in Egypt by causing harm to both individuals and society. Programs that target a small portion or just one aspect do not effectively combat obesity. Ecological and community-based solutions need to be implemented to combat obesity a growing epidemic. A combination of diet modification, in addition to increased physical activity and behavior therapy, can be effective (National Institute of Health, 2000). Key elements for effective programs working on preventing obesity need to be considered. There is little focus on obesity in Egypt. There is a strong need for obesity prevention programs. Recommendations from research should be taken into consideration. There is some hope regarding the new national strategy for nutrition. Collaboration in obesity prevention programs, nationwide campaigns and having obesity on the government’s agenda is of utmost priority. Obesity has become an alarming epidemic in Egypt by causing harm to both individuals and society. Programs that target a small portion or just one aspect do not effectively combat obesity. Ecological and community-based solutions need to be implemented to combat obesity a growing epidemic. A combination of diet modification increased physical activity and behavior therapy can be effective (National Institute of Health, 2000). Key elements for effective programs working on preventing obesity need to be considered.
Acknowledgments
The author would like to thank Dr. Rhonda K. Lewis for her constant support and supervision to finalize the publishing of this article. Her support, comments, reviews and insightful suggestions of the manuscript are the reason for the completion of this article. The original study was supported by Dr. Carie Forden and Dr. Amy Carillo; I am grateful for all their efforts, motivation, continuous support, guidance and patience. Without them I could not have imagined going through this journey.
References
Agency for Healthcare Research and Quality (AHRQ). (2013). Childhood Obesity Prevention Programs: Comparative Effectiveness Review and Meta-Analysis. Comparative Effectiveness. Rockville, MD: Wang, Y., Wu, Y., Wilson, R. F., Bleich, S., Cheskin, L., Weston, C., Showell, N., Fawole, O., Lau, B., Segal, J.; June 2013. Retrieved from www.effectivehealthcare.ahrq.gov/reports/final.cfm
Aitsi-Selmi, A., Chandola, T., Friel, S., Nouraei, R., Shipley. M.J., & Marmot, M. G. (2012). Interaction between education and household wealth on the risk of obesity in women in Egypt. PloS one,7(6), Retrieved from: http://www.plosone.org/article/fetchObject.action?uri=info%3Adoi%2F10.1371%2Fjournal.pone.0039507&representation=PDF.
Alpert, P. T. (2009). Obesity: A worldwide epidemic. Home Health Care Management Practice, 21, 442-444.
Arrizza, N. (2005). The obesity self-esteem cycle. Ezine Articles. Retrieved from http://ezinearticles.com/?The-Obesity-Self-Esteem-Cycle&id=111333.
Asfaw, A. (2006). The effects of obesity on doctor-diagnosed chronic diseases in Africa: empirical results from Senegal and South Africa. Journal of Public Health Policy, 27(3), 250-264.
Asfaw, A. (2007). Do government food price policies affect the prevalence of obesity? Empirical evidence from Egypt. International Food Policy Research Institute (IFPRI), 35(4), 687–701.
Atinmo, T., Mirmiran, P., Oyewole, O.E., Belahsen,R., & Serra-Majem, L.(2009). Breaking the poverty/malnutrition cycle in Africa and the Middle East. Nutrition Reviews. 67 Suppl 1:S40-6. doi: 10.1111/j.1753-4887.2009.00158.x
Bacon, L., Keim, N. L., Van Loan M. D., Derricote,M., Gale, D., Kazaks, A.,& Stern, J. S. (2002). Evaluating a 'non-diet' wellness intervention for improvement of metabolic fitness, psychological well-being and eating and activity behaviors. International Journal of Obesity, 26(6), 854-865.
Becton, L., Shatat, I. & Flynn, J. (2012). Hypertension and obesity: epidemiology, mechanisms and clinical approach. The Indian Journal of Pediatrics,79(8), 1056–1061.
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32(7), 513-531.
Campbell, M., Sahin-Hodoglugil, N. N., & Potts, M. (2006). Barriers to fertility regulation: a review of the literature. Studies in Family Planning. Retrieved from: http://www.ncbi.nlm.nih.gov/pubmed/16832983
Cohen, L., Perales, D. P., & Steadman, C. (2005). The O Word: Why the Focus on Obesity is Harmful to Community Health. Californian Journal of Health Promotion. 3(3), 154-161.
Colditz, G. A. (1992). Economic costs of obesity. The American Journal of Clinical Nutrition,55(2), 503S–507S.
Cosoveanu, S., Bulucea, D. (2011). Obesity in children – an increasing pediatric issue. Romanian Journal of Pediatrics, 60(2).
De Negri, B. & Thomas, E. (2003). Making sense of focus group findings: A systematic participatory analysis approach. Washington, DC: Academy for Educational Development.
Devaux, M., Sassi, F., Church, J., Cecchini, M., & Borgonovi, F. (2011). Exploring the relationship between education and obesity. OECD Journal: Economic Studies, Vol.2011/1. Retrieved from http://dx.doi.org/10.1787/eco_studies-2011-5kg5825v1k23
Dey, I. (1993). Creating Categories. In Qualitative Data Analysis: A user-friendly guide for social scientists. London and New York: Routledge.
El Baba, M., (2012). 'Obesity'. In: Elzouki, A. Y., Harfi, H. A., Nazer, H. M., Stapleton,F. B., Oh, W., Whitley, R. J. (ed), Textbook of Clinical Pediatrics. 1st ed. USA: Springer Berlin Heidelberg. pp. (769-777).
Ellabany, E. & Abdel Nasser, M.A. (2006). Non- Communicable Disease Surveillance System, Egypt 2006. Ministry of Health and Population. Preventive and Primary Health Care Sector Preventive Sector. Retrieved from http://www.who.int/chp/steps/EgyptSTEPSPresentation.pdf
Epstein, L.(1996) Family-based behavioural intervention for obese children. International Journal of Obesity and Related Metabolic Disorders: Journal of the International Association for the Study of Obesity, 20 (1).
Farooqi, I. (2006). Genetic aspects of severe childhood obesity. Pediatric Endocrinological Review, 3, 528-536.
Ferrara, C. M. (2009). The college experience: Physical activity, nutrition, and implications for interventions and future research. Journal of Exercise Physiology online. Retrieved from: https://www.asep.org/asep/asep/Ferrara%2012(1)23-35.doc
Folta, S. C., Goldberg, J. P., Economos, C., Bell, R., & Meltzer, R. (2006). Food advertising targeted at school-age children: A content analysis. Journal of Nutrition Education and Behavior, 38, 244 –248.
Food and Agriculture Organization of the United Nations (FAO). (2005). The state of food and agriculture. Agricultural trade and poverty can trade work for the poor? FAO Agriculture Series No. 36.
Food and Agriculture Organization of the United Nations (FAO). (2006). The double burdenof malnutrition: Case studies from six developing countries. Rome. Retrieved from http://www.fao.org/docrep/009/a0442e/a0442e00.htm.
Frumkin H. (2006) Introduction: Safe and Healthy School Environments. In: Frumkin H, Geller RJ, Rubin IL, Nodvin J, (Eds.), Safe and Healthy School Environments New York: Oxford University Press
Garasky, S., Stewart, S., Gundersen, C., Lohman, B. & Eisenmann, J. (2009). Family stressors and child obesity. Social Science Research, 38(4), 755–766.
Geier, A. B., Schwartz, M. B., & Brownell, K. D. (2003). "Before and after" diet advertisements escalate weight stigma. Eating and Weight Disorders; 8(4): 282–288.
General Motors Diet. (2015). Retrieved from http://www.generalmotorsdiet.net/
Georgetown University Center on an Aging Society. (2002). Childhood obesity: A lifelong threat to health. [Data Profile]. Retrieved from http://hpi.georgetown.edu/agingsociety/pdfs/obesity.pdf
Glanz, K., Sallis, J. F., Saelens, B. E., & Frank, L. D. (2005). Healthy nutrition environments: Concepts and measures. American Journal of Health Promotion,19(5): ii, 330-333.
Glanz, K., Sallis, J. F., Saelens, B. E., & Frank, L. D. (2007). Nutrition environment measures survey in stores (NEMS-S): Development and evaluation. American Journal of Preventive Medicine. 32(4):282-289.
Gleason, P., Suitor, C. (2001). Food for thought: Children's diets in the 1990s. Princeton, N.J.: Mathematica Policy Research, Incorporated.
Gobo, G. (2003). Sampling, Representativeness and Generalizability, 3110 (28), 435.
Golan, M., Crow, S. (2004). Targeting Parents Exclusively in the Treatment of Childhood Obesity: Long-Term Results. Obesity Research, 12(2). Retrieved from http://onlinelibrary.wiley.com/doi/10.1038/oby.2004.45/full
Grier, S., & Kumanyika, S. K.(2008). The Context for Choice: Health Implications of Targeted Food and Beverage Marketing to African Americans. American Journal of Public Health; 98(9): 1616–1629.doi: 10.2105/AJPH.2007.115626. Retrieved from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2509618/
Hadley, A. M., Hair, E. C., & Dreisbach, N. Child Trends (2010) What works for the prevention and treatment of obesity among children: Lessons from Experimental Evaluations of Programs and Interventions (Publication No 2010-07 4301) Washington, DC. Retrieved from: www.childtrends.org.
Hajhosseini, L., Holmes, T., Mohamadi, P., Goudarzi, V., McProud, L. & Hollenbeck, CB. (2006). Changes in body weight, body composition and resting metabolic rate (RMR) in first-year university freshman students. Journal of American College of Nutrition, 25(2), 123-137.
Hassan, H., Moussa, W. & Ismail, I. (2005) Assessment of dietary changes and their health implications in countries facing the double burden of malnutrition: Egypt, 1980 to 2005. The double burden of malnutrition, 43. Retrieved from http://www.fao.org/docrep/009/a0442e/a0442e07.htm.
HSC Foundation. (2009). Fighting Obesity: What Works, What’s Promising. Washington, DC: Elliot A. Segal. Retrieved from:http://www.hscfoundation.org/aboutus/publications/Fighting%20Obesity%20Report.pdf.
Hu, F. (2008). Genetic predictors of obesity. Obesity Epidemiology, 64, 437.
Hudd, S., Dumiao, J., Erdmann-Sager, D., Murray, D., Phan, E., Nicholas, S., Yokozuka, N. (2000). Stress at College: effect on health habits, health status and self-esteem. College Student Journal,34(2).
Huhman, M., & Patnode, C. D. (2013). Communities leveraging the assets of a national social marketing campaign: Experiences with VERB. It’s what you do! Springer Science+Business Media.
International Association for the Study of Obesity (IASO). (2010). Obesity: Understanding and challenging the global epidemic: 2009-2010 Report. Retrieved from http://www.iaso.org/site_media/uploads/IASO_Summary_Report_2009.pdf.
International Association for the Study of Obesity (IASO). (2012). [Graphic illustration using a world map] Global prevalence of obesity in adult females. Retrieved from http://www.iaso.org/site_media/library/resource_images/Global_Obesity_Top_5_in_each_region.pdf.
Jackson, R. T., Rashed, M., & Saad-Eldin, R. (2003). Rural urban differences in weight, body image, and dieting behavior among adolescent Egyptian Schoolgirls. International Journal of Food Sciences & Nutrition, 54(1), 1.
Kime, N. (2008). Children's eating behaviours: the importance of the family setting. Area, 40(3). Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1475-4762.2008.00834.x/full.
Larson, N. I., Story, M. T., & Nelson, M. C. (2009). Neighborhood environments: disparities in access to healthy foods in the US. American Journal of Preventive Medicine, 36(1), 74-81.
Lawlor, D., Smith, G., & O’Callaghan, M. (2007). Epidemiologic evidence for the fetal overnutrition hypothesis: findings from the mater-university study of pregnancy and its outcomes. American Journal of Epidemiology, 165(4), 418–24.
Major, B., Eliezer, D., &Rieck, H. (2012). The psychological weight of weight stigma. Social Psychological and Personality Science, 3(6), 651-658.
National Academy of Sciences. (2013). Evaluating Obesity Prevention Efforts: A Plan for Measuring Progress Committee on Evaluating Progress of Obesity Prevention Efforts. Washington, DC:Green, L. W., Sim, L., & Breiner, H. Retrieved from: http://www.acsh.org/wp-content/uploads/2013/08/18334.pdf
National Institute of Health. (2000). The Practical Guide Identification, Evaluation,and Treatment of Overweight and Obesity in Adults. Retrieved from https://www.nhlbi.nih.gov/files/docs/guidelines/prctgd_c.pdf
Owen, C., Martin, R., Whincup, P., Smith, D., & Cook, D. (2005). Effect of infant feeding on the risk of obesity across the life course: a quantitative review of blished evidence. Pediatrics, 115(5), 1367–1377.
Pervanidou, P. & Chrousos, G. (2011). Stress and obesity/metabolic syndrome in childhood and adolescence. International Journal of Pediatric Obesity, 6(S1), 21–28.
Prilleltensky, I., Nelson, G., Peirson, L. (2001). Promoting family wellness and preventing child maltreatment: Fundamentals for thinking and action. Toronto: University of Toronto Press.
Racette, S., Deusinger, S., Strube, M., Highstein, G. & Deusinger, R. (2005). Weight changes, exercise, and dietary patterns during freshman and sophomore years of college. Journal of American Collage Health,53 (6), 245-251.
Ravussin, E., &Swinburn, B. (1992). Pathophysiology of obesity. The Lancet, 340(8816), 404-408.
Renzaho, A. M.N. (2004). Fat, rich and beautiful: changing socio-cultural paradigms associated with obesity Risk, nutritional status and refugee children from Sub-Saharan Africa. Health & Place, 10(1), 105-113.
Salazar-Martinez, E., Lazcano-Ponce, E., Sanchez-Zamorano, L., Gonzalez-Lira, G., Escudero-De Los Rios, P. & Hernandez-Avila, M. (2005). Dietary factors and endometrial cancer risk. Results of a case–control study in Mexico. International Journal of Gynecological Cancer, 15: 938–945.
Seo, D., & Sa, J. (2010). A meta-analysis of obesity interventions among U.S. minority children. Journal of Adolescent Health, 46(4), 309-323.
Shahin, H. (2015) obesity interventions in Egypt: Identifying gaps and highlighting assets (Master’s Thesis). The American University in Cairo, Cairo, Egypt.
Singh, A. S., Mulder, C., Twisk, J. W. R., Twisk, C., Van Mechelen, W., &Chinapaw, M. J. M. (2008) Tracking of childhood overweight into adulthood: a systematic review of the literature. International Association for the Study of Obesity, 9(5), 474-488.
Sobko, T., Svensson, V., Ek, A., Ekstedt, M., Karlsson, H., Johansson, E., Cao, Y., Hagströmer, M., & Marcus, C. (2011). A randomised controlled trial for overweight and obese parents to prevent childhood obesity - EarlySTOPP (Stockholm Obesity Prevention Program). BMC Public Health, 11(1), 336.
Sturm, R. (2002). The effects of obesity, smoking, and drinking on medical problems and costs. Health Affairs, 21(1), 245-253.
Summerbell, C. D., Waters, E., Edmunds, L., Kelly, S., Brown, T., & Campbell, KJ. (2005). Interventions for preventing obesity in children. Cochrane Database System Reviews, 3 (3).
Ternouth, A., Collie, D., Maughan, B. (2009). Childhood Emotional Problems and Self-perceptions Predict Weight Gain in a Longitudinal Regression Model. BMC Medicine, 7, 46.
Traill, B. (2006). Trends towards overweight in lower- and middle-income countries: some causes and economic policy options. FAO Food and Nutrition Papers. Retrieved: http://www.fao.org/docrep/009/a0442e/a0442e0x.htm.
Veerman, J.L. (2011). On the futility of screening for genes that make you fat. PLoS Medicine, 8(11).
Wang, F., Wild, T., Kipp, W., Kuhle, S., &Veugelers, P. (2009). The influence of childhood obesity on the development of self-esteem. Statistics Canada 20(2). Retrieved from http://www.statcan.gc.ca/pub/82-003-x/2009002/article/10871-eng.pdf.
Withrow, D., & Alter, D. A. (2010). The economic burden of obesity worldwide: a systematic review of the direct costs of obesity. Obesity Reviews, 12(2), 131-141.
World Health Organization (WHO). (1997). Obesity: Preventing and managing the global epidemic. Geneva: World Health Organization.
World Health Organization (WHO). (2000). Obesity: Preventing and managing the global epidemic (No. 894). Geneva, Switzerland: World Health Organization.
World Health Organization (WHO). (2003). Global strategy on diet, physical activity and health. Retrieved from www.who.int/dietphysicalactivity/en/.
World Health Organization (WHO). (2008). World Health Statistics 2008. Geneva, Switzerland: World Health Organization.
World Health Organization (WHO). (2009). Global Health Risks Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva, Switzerland: World Health Organization.
World Health Organization (WHO). (2010). World Health Statistics 2010. Geneva, Switzerland: World Health Organization.
Zulet M. A., Berkenpas M. E., & Martinez, J. A. (2005). Comparison of dietary approaches to treat obesity based on the different carbohydrate/fat content: Impact on weight loss and lipid profile. Current Nutrition & Food Science, 1(1).
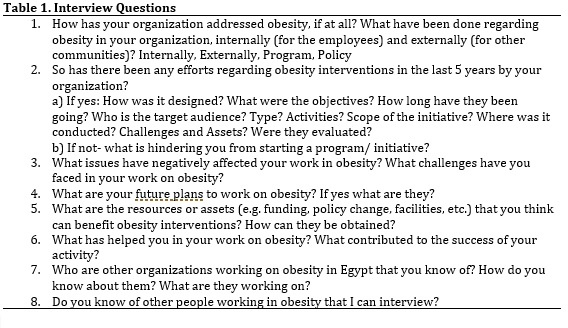 Table1.Interview Questions |
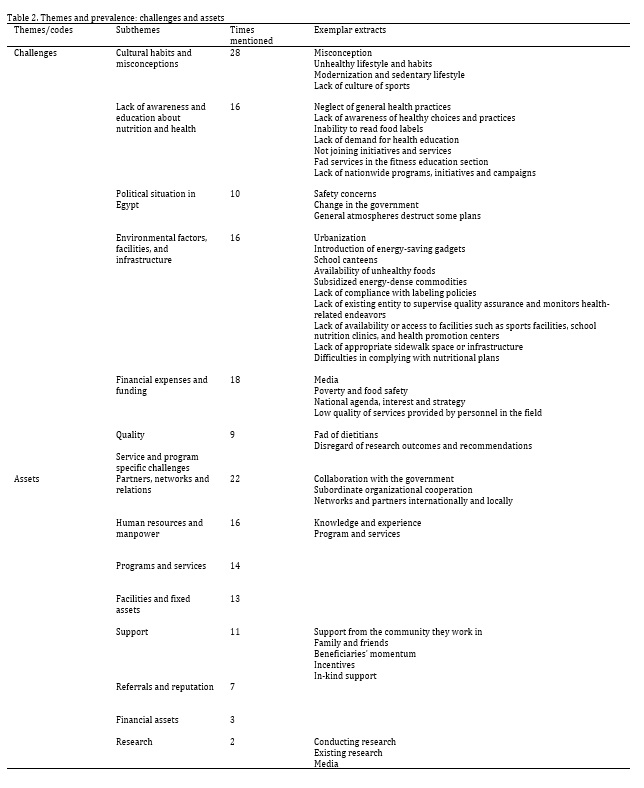 Table2.Themes and prevalence:challenges and assets |
 Figure1.Map of Egypt |
 Hana Shahin
Hana Shahin
Hana Shahin, community psychologist with a master’s degree from the American University in Cairo (AUC) and a master’s degree from Wichita State University. She has had over ten years of experience with youth development and cross-cultural understanding, and community development organizations. Currently, she is a doctoral candidate at Wichita State University and a freelance consultant in community psychology, organizational development, and capacity building.
agregar comentario
![]() Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
palabras clave: Obesity, ecological framework, obesity programing and interventions, recommendations for obesity programming, and Egypt.
 Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.
Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.
