



In this manuscript, the author draws from her experiences on a South Carolina educational-research obesity initiative to describe the important value that community psychology (CP) brings to medical education and healthcare organizations. The article describes the set of CP competencies that were most influential to the initiative and discuss how those competencies shaped the course of the initiative. More specifically, the author discusses: 1) how the use of a participatory action research approach helped ground project efforts in the practical realities of the participating practices, 2) how the team developed sociocultural and cross-cultural competence to better understand the complexity of weight-related issues in healthcare, and 3) how using an ecological perspective facilitated practice-wide improvements in obesity management. Through a series of examples, the article highlights specific ways medical education organizations can leverage community psychology competencies to move beyond traditional continuing medical education (CME) methods.
Download the PDF version to access complete article, including Tables and Figures
In her mid-50s, Brittany woke up one morning and noticed a dull pain in her left knee. She shrugged it off and continued her weekday routine of getting ready for work. Over the course of six months, the knee pain gradually intensified. Brittany began avoid stairs and hills, which seemed to make her knees hurt even more. Already obese and self-conscious about her weight, Brittany noticed that she had gained eight pounds since her left knee started to hurt. After talking with a friend about the knee pain and her weight gain, she decided to schedule an appointment with her primary care doctor.
Brittany’s time in the waiting room was longer than she would have liked; however, her appointment with Dr. Bradley was quick and easy. He told her knee pain was a common symptom for persons who were heavy set, prescribed painkillers, and asked her to schedule a follow-up visit for two weeks out. Brittany was not happy to learn that her weight was impairing her left knee, but she was glad to have a remedy for the pain.
Two weeks later, Brittany had to reschedule her doctor’s appointment due to an unexpected change in her work schedule. Dr. Bradley was booked three weeks out, and so Brittany scheduled to see another physician at the primary care practice.
During the follow-up appointment, Brittany met with Dr. Vera. She was surprised by Dr. Vera’s interest in her weight. Dr. Vera asked about her lifestyle, what she ate, the kind of neighborhood she lived in, and what she liked to do for physical activity. She asked Brittany how she felt about her weight and how motivated she was to lose weight. Although Brittany was generally very private about her weight-related concerns, she found it surprisingly easy to talk with Dr. Vera. After the conversation, Dr. Vera gave Brittany an exercise prescription and took her off the painkillers. Dr. Vera believed that Brittany’s knee pain would dissipate with exercise and weight loss. Brittany was relieved to be able to talk with a professional about her weight. She was unsure about stopping the painkillers, but excited about starting a swimming routine.
One month later, Brittany had dropped seven pounds She had almost lost all the weight that was put on since the knee pain started, but was frustrated to still have the pain in her left knee. She called the doctor’s office again. The receptionist scheduled her to see Dr. Bradley.
During the appointment, Dr. Bradley was flushed with annoyance to learn that Brittany had stopped taking her pain medication. She proudly shared her new exercise regime and weight loss with Dr. Bradley. Dr. Bradley responded indifferently. He told Brittany that she should stay on her pain medication if she wanted the pain to go away. He explained that trying to lose weight at her age was very difficult, and that most obese patients are not successful with maintaining weight loss.
Brittany left the doctor’s office feeling confused and deflated. Should she bother to exercise? Should she start her pain medication again? Why were the doctors giving her such conflicting messages and prescriptions?
Nearly three-quarters of adults in the United States (U.S.) are overweight or obese, with obesity affecting more than one-third of this population (National Center for Health Statistics, 2015). South Carolina has the tenth highest adult obesity rate in the nation at 32% (Levi, Segal, Rayburn, & Martin, 2015). Given the diverse set of medical problems associated with obesity, primary healthcare settings are critical for the successful proactive management of obesity; however, many primary care physicians report feeling uncomfortable or insufficiently competent to talk with patients about their weight-related issues (Kaminsky & Gadaleta, 2002; Anderson et al. 2001; Davis, Shishodia, Taqui, Dumfeh, & Wylie-Rosett, 2008). For example, a study of 620 family physicians revealed that 51% felt they lacked the knowledge and skill to discuss weight-related behavior changes with their patients (Huang et al., 2004). Additionally, providers vary widely in their attitudes about obesity, including whether they believe their patients can successfully lose and maintain weight loss (Anderson et al., 2001; Block, DeSalvo, & Fisher, 2003). As in the case with Drs. Bradley and Vera in the opening scenario, disparate physician attitudes about obesity complicate obesity management and interfere with desired patient health outcomes.
Enactment of the Patient Protection and Affordable Care Act (P.L.11-148) has catalyzed significant and rapid changes in the healthcare landscape in the United States. Healthcare systems have elevated their interest in improving care quality, lowering healthcare costs, and achieving patient and population health outcomes (Mann, 2010). In addition, rather than volume-based care models, pay-for-performance structures are now driving reimbursement levels as a means of promoting quality outcomes. To evolve with changing industry demands, healthcare systems across the nation are re-examining their practices and embracing alternative approaches. For example, services are shifting from provider-led to patient-centered care. Healthcare settings are adopting and using electronic healthcare records to track and measure patient outcomes. And the philosophy of quality improvement and lean management is more vigilantly applied across operational levels. These sweeping changes are directly impacting medical education organizations, compelling medical educators to re-assess the way they go about their work and to question the adequacy of existing continuing medical education (CME) structures, supports, and methods for preparing physicians to provide safe, quality patient care.
Along these lines, medical educators are moving away from traditional approaches to education--where educational activities are largely didactic, episodic, in the classroom, and focused on the individual--to approaches that promote ongoing, team-based learning in settings that simulate or represent real work conditions. Medical educators are turning to implementation science to better understand what educational interventions work where, when, how, and for whom (Carney et al., 2016; Price et al., 2015). They are asking fundamental questions about ways medical education can contribute to more meaningful educational outcomes. In tandem with these shifts has been an increased recognition of the value that interdisciplinary education and multi-organizational collaboration can bring to quality improvement efforts.
In 2011, the University of South Carolina School of Medicine CME Organization partnered with the Medical University of South Carolina CME Organization to implement a multi-year educational-research initiative aimed to improve the quality of obesity healthcare. Referred to as the South Carolina Initiative for Quality Overweight/Obesity Care (SCIQOC), this pilot initiative was designed to move beyond traditional CME formats (i.e., didactic lectures, case conferences) toward an educational approach targeting organizational-level improvements. During this exploratory journey, the competencies of community psychology played a pivotal role in designing, planning, and implementing SCIQOC.
In this manuscript, the author draws from her experiences with SCIQOC to describe the important value that community psychology (CP) skills bring to medical education and healthcare organizations. Specifically, this article focuses on three community psychology competencies that critically influenced the course of the initiative: participatory action research, sociocultural and cross-cultural competence, and ecological perspectives. Through a series of examples, the article highlights specific ways medical education organizations can leverage community psychology competencies to move beyond traditional CME methods.
Background: SCIQOC Participants and Project Design
The obesity initiative included two primary care practices situated in urban settings of South Carolina. At project start, Primary Care Practice A included 15 clinicians, 24 clinical staff members (nurses, nurse assistants), and 15 patient service representatives (front staff). Primary Care Practice B had 5 clinicians, 2.5 clinical staff members, and 3 front staff.
SCIQOC involved a two-stage assessment phase (exploratory assessment and needs assessment), followed by an intervention phase (see Figure 1). The exploratory assessment entailed a literature review and separate focus groups with overweight and obese persons, community providers, and primary care providers not affiliated with participating practices.
Figure 1: SCIQOC Design (See PDF version or image below)
This preliminary assessment helped the SCIQOC team understand issues from both a science (evidence-based) and local perspective. The needs assessment included: a) an obesity healthcare questionnaire administered to practice staff and physicians; b) a focus group involving clinical and administrative staff; c) a semi-structured interview with practice leaders; and d) an environmental assessment involving clinic setting observations, clinical mapping checklist, and patient simulations. The needs assessment aimed to identify practice gaps within each participating practice. Additional information about the exploratory and needs assessment is provided in Table 1. The obesity initiative was supported by grant funding from Pfizer Independent Grants for Learning & Change (#034452).
Table 1: Summary of SCIQOC Assessment Stages (See PDF version or image below)
Using a Participatory Action Research Approach to Ground Our Work in the Practical Realities of Participating Healthcare Organizations
While a participatory action research design is more time-intensive than an investigator-led design, SCIQOC leadership (PI and Project Director) believed it was essential to work closely with practice members in order to make meaningful local improvements in obesity healthcare. We actively turned to practice members for insights into the challenges of obesity healthcare and trusted they were best positioned to generate practical solutions to address existing local challenges. This section describes how we used a participatory approach across the phases of SCIQOC.
Grant Preparation
Our engagement with the participating practices began during the grant preparation stage of the initiative. We met with practice leadership to address project issues such as: Who will benefit from the obesity initiative and in what ways? What type of commitment is needed from the practices to improve obesity care quality? Which members will actively champion the effort? What are existing and anticipated resource needs (staff, financial, technical)? How will interventions be sustained? During this early stage of engagement, we found that having pre-existing relationships with members of the practice facilitated open, frank conversations about ongoing challenges and limitations with addressing obesity. For example, practice members expressed concern about the weight of their own healthcare teams and how being obese could impact provider motivation to improve obesity care quality.
Assessment Phase
Upon successful grant funding, the SCIQOC team worked with appointed practice members to determine questions for the assessment phase. For instance, to develop the focus group and interview questions, the SCIQOC team drafted initial questions, which were sent to practice members for review. We used an iterative “review, discuss, refine” process to finalize the qualitative instrument. To develop the obesity questionnaire, practice members and the research team pooled and reviewed survey instruments. Questionnaires were vetted based on psychometric properties and alignment with the aims of the initiative.
Intervention Phase
After analyzing the needs assessment data, the SCIQOC team held a series of meetings with practice leadership and one in-person, practice-wide meeting. The meetings involved discussions about the assessment data, selection of priority practice gaps, and review of evidence-based strategies and programs for addressing existing needs. The goal of the meetings was to determine the most fitting intervention strategies and/or programs for each practice based on its needs and capacities as well as the costs and benefits of the interventions. The process for choosing intervention strategies was highly collaborative, involving practice leadership, physicians, clinical staff, and administrative staff. During each meeting with practice members, SCIQOC team members served primarily as facilitators. We listened attentively and guided the conversation per agreed upon meeting objectives. Where useful, we researched and provided additional information.
The process of sharing decision-making about the set of intervention activities was difficult for some members of the SCIQOC educational-research team (comprised of individuals from the University of South Carolina and the Medical University of South Carolina) who were partial to particular intervention strategies. This fostered emotional tension and short-term disengagement from select team members. As an educational-research team, we worked through this disruption by exploring the rationale and emotions underlying existing views. The open conversations provided discontent team members a fuller understanding of the distinction between participatory and non-participatory research approaches. The conversations helped SCIQOC team members develop a better sense of what it “looks, feels, and sounds like” to share decision-making with members of the participating practices. Later, into the intervention phase, the benefits of shared decision-making become apparent to those SCIQOC team members who originally resisted the approach.
Overall, the participatory approach made it possible for both SCIQOC team members and project participants to develop not only an intellectual understanding of issues, but also a socio-emotional understanding. The participatory approached helped us ground our efforts in the practical realities and emotional challenges of addressing obesity. Working with practice members made it possible for interventions to be tailored specifically to the needs of each practice (rather than providing a standard, pre-determined educational program as is typically provided via CME). Simultaneously, practice members gained a greater appreciation for data and were better positioned to make data-informed decisions. They were engaged throughout the initiative and had ownership over its trajectory. An unanticipated but celebrated outcome of the participatory approach is that it fostered opportunities for additional communication among healthcare team members, which improved patient coordination by surfacing practice gaps.
Developing and Exercising Sociocultural and Cross-Cultural Competence to Understand the Complexity of Weight-related Issues in Healthcare
Culture shapes our perceptions and guides human behavior. As a society, the U.S. has an individualistic orientation, prizing self-reliance, independence, and achievement. Although a host of historical, contextual, and circumstantial factors (e.g., our upbringing, surrounding environment, access to resources and opportunities) influence obesity, it is often viewed as an individual-level issue. American society tends to blame obese persons for their weight-related problems. To improve obesity healthcare quality the SCIQOC team needed to be conscious and transparent about our own views of obesity and obese persons.
Sociocultural and cross-cultural competence involves the ability to value, integrate, and bridge multiple worldviews, cultures, and identities (Dalton & Wolfe, 2012). From the beginning of SCIQOC, the team committed to being open and honest with one another in our conversations. A critical first step toward fostering sociocultural and cross-cultural competence among the team was developing self- and collective awareness about our own views of obesity and pertinent associated dimensions of diversity (e.g., race, ethnicity, social class, locality). Individually, each SCIQOC team member completed a series of implicit attitudes tests on weight, race, and gender (see https://implicit.harvard.edu/implicit/takeatest.html). Then, collectively, we discussed the results and implications of our biases for our work. We viewed biases as natural, but modifiable human tendencies. At project start, we also reflected openly on our assumptions about obesity and the local population. This process of conscious raising shed light on the boundaries of our socio-cultural knowledge and served as a springboard for the exploratory assessment with local participants.
The SCIQOC team was diverse in educational and training background. The team included a community psychologist (author), with training in business and clinical-community psychology; a political scientist; a health psychologist; a physician, and other individuals with backgrounds in the health and human services industry. All members of the leadership team were nested in continuing medical education organizations and responsible for any array of professional development activities. The team was also diverse in age (ranging from 25 to 70 years), gender, and race/ethnicity (Asian American, Jewish, Ghanaian, White/Caucasian). However, the team’s characteristics did not closely mirror the population of obese persons, who tended to be lower socioeconomic status and black, African American or Latino/a. In preparing for the focus groups, we were sensitive to these differences and mindful of our “outsiderness”. We addressed this cross-cultural challenge with humility and transparency. During the focus groups, we explicitly noted the cross-cultural differences, listened open-mindedly, and invited participants to “correct” our language where useful. To focus conversations on the issues (rather than persons), questions were largely framed in the third person (e.g., Do you have a family or friend who sees the doctor because of weight-related problems? What are her/his experiences?). We found the use of a third person frame for raising questions to be highly effective for broaching sensitive topics relating to obesity. Participants were eager to share stories about the weight-related healthcare experiences of their family and friends, and these stories naturally led to energetic discussions about personal challenges with weight-related issues (e.g., the stigma of being overweight; delays in seeking treatment for weight-related healthcare issues, such as diabetes or hypertension, due to fear of being scolded by one’s doctor about being overweight; balancing the desire to lose weight with concerns about losing friendships if one becomes thin). Together, these methods fostered focus group conversations that were deep, generative, and meaningful.
The SCIQOC team viewed the development of cross-cultural competence as a “life-long” process. Through this orientation, team members were encouraged to raise questions about race, weight, and other sensitive topics. We asked these questions not only of each other, but also of SCIQOC participants (obese persons, community health providers, and primary care providers). Such questions helped the SCIQOC team understand the complexity of issues impacting obesity and obesity healthcare. For example, the process of open inquiry shed light on the central role of religion/spirituality in how some individuals viewed their weight (e.g., “this is the size God wants me to be”; “I leave my weight up to God.”). Through first-hand accounts by both physicians and obese patients, we also heard the need for greater sociocultural competence in obesity healthcare. Physicians shared their discomfort with talking about weight, particularly with individuals of different races/ethnicities and gender. Patients described physicians as lacking understanding of the patient’s culture and life circumstances. For instance, one African American patient explained that a physician instructed her to engage in vigorous cardio aerobics (e.g., running), which did not align with the patient’s lifestyle. She explained that it took 4-8 hours to have her hair done, and that having her hair done was expensive. Vigorous cardio aerobics was not a viable weight management option because it would cause her to sweat and ruin the weaves in her hair. She also explained that her physicians never talk with her about her life and how her lifestyle affected her weight; instead, “they just tell me to lose weight”. We found these personal, sensitive stories were at the heart of knowing how to improve obesity care quality. Such stories were elicited by broaching the range of sociocultural topics with an open-mind and listening with humility. We experienced an “easing in”, where the more we talked about the topics of race, social class, and weight, the more natural and comfortable the conversations felt.
In the needs assessment stage of SCIQOC we learned that cultural and racial biases about obese persons were pervasive within participating practices. These biases had never been explicitly discussed, although they would occasionally “slip out” in negative terms during conversations among providers. After the needs assessment, a practice-wide meeting was scheduled with each participating primary care practice to discuss assessment results and next steps. During the meeting, we invited practice members to reflect on how well the data mirrored the views and patterns of the practice. We listened with openness, while attending to the distribution of power within the room. We were mindful of the hierarchical structure of healthcare and how power structures could impact who had voice in the room.
In hindsight, the method by which our team developed sociocultural and cross-cultural competence closely tracks with Balcazar and colleagues’ (2009) training model for cultural competence, which begins at the individual level and expands outward. Their model captures the following stages: desire to engage, development of critical awareness of personal biases toward others who are different, development of knowledge about issues of diversity and culture, development and practice of skills for working across cultural groups, and working toward organizational/broader societal support for cultural competence. As reflected in the developmental approach by Balcazar and colleagues (2009), we found it was critical to foster sociocultural and cross-cultural competence from the inside out, starting with personal reflection (intra-study) and then engaging dialectically across the ecological levels.
Leveraging the Systems Perspective to Facilitate Practice-based Improvement
We entered this project with the premise that educating the healthcare team was necessary, but not sufficient for improving obesity care quality. Individual experiences are embedded in a context, which influences behavior and outcomes (Brofennbrenner, 1977; Kelly, Ryan, Altman, & Stelzner, 2000). Patient healthcare experiences are shaped by the totality of their interactions with the healthcare practice. This includes tangible and intangible aspects of the healthcare system (e.g., ease of scheduling an appointment, layout of the waiting room, patient flow process, and adequacy of the healthcare equipment). Our conversations with patients and providers during the exploratory assessment underscored the impact of contextual factors on both patient and provider experiences with obesity care. Patients shared stories of feeling embarrassed when blood pressure cuffs were too small to fit around their arms and when exam room tables were not sturdy enough for their body weight. Providers raised concerns about the location of the scales and questioned whether patients were comfortable having their weight taken in such a high foot traffic area.
To deepen our understanding of the practice environment, the needs assessment was designed to attend to operational, physical, and sociocultural aspects of the practices. Serving as simulation patients, SCIQOC team members participated in a doctor’s visit to get a feel for the patient flow process. We conducted onsite observations of practice activities. We also interviewed healthcare team members about the practice environment. This multi-method approach to studying the clinical setting helped us understand existing interdependencies (e.g., who talks to whom, who avoids whom, how administrative and clinical activities affect one another), how resources are allocated and used, power structures and dynamics, and the organizational culture (e.g., operating values, openness to innovations and change, accountability, and employee satisfaction and commitment). We learned about formal and informal processes for decision-making and how decisions were translated (or not) into implementation. Taking a systems perspective and inviting involvement from all practice members helped us learn about the responsibilities of healthcare team members as well as their skills, talents, and interests. As the initiative moved into implementation, this knowledge was useful for ensuring we had the “right” members in the “right seat” on the “right bus”. By involving all practice members (rather than just physicians as is typical in traditional CME approaches), we obtained a well-rounded sense of the issues salient to obesity healthcare. As expected, we also found that practice-wide involvement during the needs assessment facilitated member engagement (buy-in) during the intervention phase.
Conclusion
In the interest of moving away from traditional CME formats, SCIQOC was a pilot effort to develop an educational approach that would result in more impactful and sustainable obesity healthcare outcomes for primary care practices. The three community psychology competencies (participatory action research, sociocultural and cross-cultural competence, and ecological perspective) described in this article were invaluable both for thinking “outside” and “inside” the box in terms of CME formats, clinical settings, and patient needs. Working closely with the practices to design, plan, and implement the phases of SCIQOC ensured that meaningful and relevant questions were being asked and that selected interventions “fit” the practice environment. The process of sharing decision-making over an extended period of time (approximately two years) provided members with multiple opportunities to reflect and weigh-in on obesity healthcare, which contributed to organizational readiness for engaging in selected interventions.
The SCIQOC initiative catalyzed a series of organizational improvements for both participating practices.
Primary Care Practice A:
During the intervention phase we were deliberate about identifying personnel who could be specifically dedicated to planning, implementation, and evaluation activities. We were also intentional about ensuring these were members who were already embedded within and familiar with the practice. Clear role expectations and leveraging intra-system resources was important for implementation and sustainability of activities.
Primary Care Practice B:
In addition to the practice improvements described above, members across both practices reported an increased understanding of general issues pertaining to obesity and obesity healthcare as well as an increased understanding of how their own practice was addressing obesity. Practice members also reported being more aware of and sensitive to the needs of overweight and obese patients than prior to SCIQOC. In sum, the obesity initiative helped participating practices make important strides in their efforts to improve obesity care quality.
Community psychology provides an array of competencies that generalize readily across settings and are highly suitable for working in dynamic, highly complex settings such as healthcare (Kirk & Neigher, 2013). Our experience with SCIQOC suggests that the competencies of community psychology (participatory action research, sociocultural and cross-cultural competence, and ecological perspective) are highly useful for designing alternative CME approaches and facilitating organizational level changes in primary care practices. To the author’s knowledge, this is the first article that examines how community psychology competencies can be practically useful for advancing medical education. Through the examples shared, the author hopes this article sheds light on the value community psychologists can bring to medical education and healthcare organizations.
References
Anderson, C., Peterson, C.B., Fletcher, L., Mitchell, J.E., Thuras, P., & Crow, S.J. (2001). Weight loss and gender: An examination of physician attitudes. Obesity Research, 9, 257-263.
Balcazar, F.E., Suarez-Balcazar, Y., & Taylor-Ritzman, T. (2009). Cultural competence: Development of a conceptual framework. Disability and Rehabilitation, 31, 1153-1160.
Block, J.P., DeSalvo, K., & Fisher, W.P. (2003). Are physicians equipped to address the obesity epidemic? Knowledge and attitudes of internal medicine residents. Preventive Medicine, 36(6). 669-675.
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32. 513-531.
Carney, P.A., Crites, G.E., Miller, K.H., Haight, M., Stefanidis, D., Cichoskikelly, E., Price, D.W., Akinola, M.O., Scott, V.C., &Kalishman, S. (2016). Building and executing a research agenda toward conducting implementation science in medical education. Medical Education Online, 21. doi: http://dx.doi.org/10.3402/meo.v21.32405.
Davis, N.J., Shishodia, H., Taqui, B., Dumfeh, C., & Wylie-Rosett, J. (2008). Resident physician attitudes and competence about obesity treatment: Need for improved education. Medical Education Online, 13(5), 1-4.
Dalton, J., & Wolfe, T. (2012). Competencies for community psychology practice. The Community Psychologist, 45(4), 7-14.
Huang, J., Yu., Marin, E., Brock, S., Carden, D., Davis, T. (2004). Physicians’ weight loss counseling in two public hospital primary care clinics. Academic Medicine, 79(2), 159-161.
Kaminsky, J. & Gadaleta, D. (2002). A study of discrimination within the medical community as viewed by obese patients. Obesity Surgery, 12(1), 14-18.
Kelly, J.G., Ryan, A.M., Altman, B.E., & Stelzner, S.P. (2000). Understanding and changing social systems: An ecological view. In J. Rappaport & E. Seidman (Eds.) Handbook of community psychology (pp. 133-159). New York, NY: Plenum.
Kirk, M., & Neigher, W. (2013). Community psychology and the future of healthcare. Global Journal of Community Psychology Practice, 4(4), 1-9.
Levi, J., Segal, L.M., Rayburn, J., & Martin, A. (2015). The State of Obesity: Better Policies of a Healthier America 2015. Trust for America’s Health/Robert Wood Johnson Foundation. Washington, D.C.
Mann S. (2010). Implementation science: A yardstick for reform. Aamc.org/newsroom/reporter/dec10/165666/Implementation_science-a-yardstick_for_reform.html. Updated 2010. (Accessed May 23, 2016)
National Center for Health Statistics. (2016). Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. Hyattsville, MD.
Price, D.W., Wagner, D.P., Krane, N.K., Rougas, S.C., Lowitt, N.R., Offodile, R.S., Easdown, L.J., Andrews, M.A.W., Kodner, C.M., Lypson, M., & Barnes, B.E. (2015). What are the implications of implementation science for medical education? Medical Education Online, 20. doi: http://dx.doi.org/10.3402/meo.v20.27003.
Download the PDF version to access complete article, including Tables and Figures
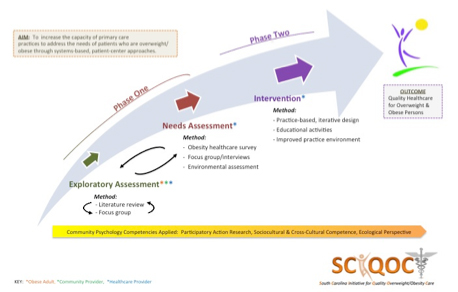 Figure 1. SCIQOC Design |
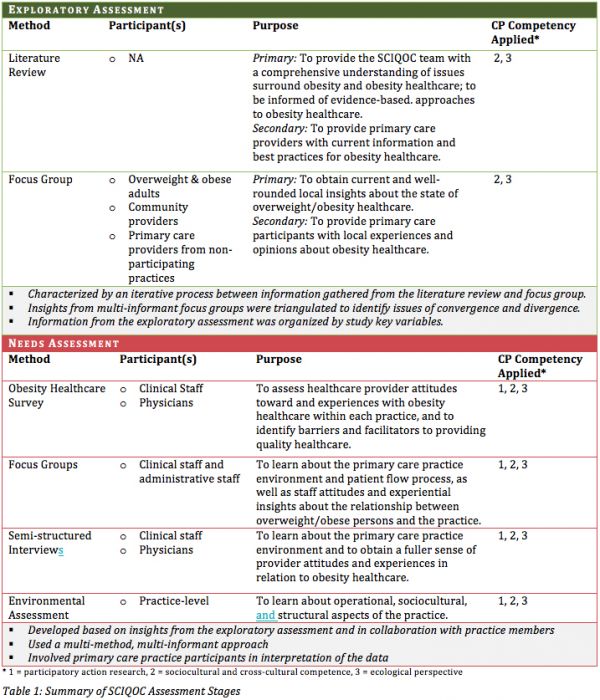 Table 1: Summary of SCIQOC Assessment Stages |
 Victoria C. Scott
Victoria C. Scott
Victoria Scott, Ph.D., MBA, is a community psychologist who has devoted her professional career to working with non-profit organizations to optimize their performance through consultation, education, research, and evaluation. Dr. Scott holds an academic appointment at the University of North Carolina Charlotte where she is an Assistant Professor of Psychology. Her research focuses on interdisciplinary approaches to improve healthcare systems and community organizations. She is particularly interested in promoting breastfeeding through hospital and workplace interventions, building organizational readiness for integrated behavioral health and primary care, and the science and art of quality improvement. In 2015, Dr. Scott received the Society for Community Research and Action Early Career Award in honor of her commitment to developing and promoting the field of community psychology. She also received the Don Klein Publication Award to Advance Community Psychology Practice for her co-edited book: Community Psychology: Foundations for Practice, which aims to further the competencies of professionals who work in community settings.
agregar comentario
![]() Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
Descargue la versión en PDF para acceder al artículo completo, incluyendo tablas y figuras.
palabras clave: community psychology competencies, continuing medical education, CME, healthcare systems, obesity healthcare
 Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.
Basado en un trabajo de www.gjcpp.org.
Los permisos que excedan el
alcance de esta licencia pueden estar disponibles en http://www.gjcpp.org/contact.php.
