


Perinatal and early childhood services are valuable resources for all new parents, particularly in supporting them as they transition to their new role. However, parents with physical disabilities report several barriers to accessing these services, including difficulty physically accessing services, lack of knowledge or negative attitudes of professionals, and lack of adaptation of services. The objective of this article is to analyse, through the Dixon-Woods et al. accessibility model, the barriers to accessing perinatal and early childhood services from the perspective of parents with physical disabilities. Thirteen semi-structured individual interviews, using the life story approach, were conducted. The results highlight barriers to access to services in all dimensions of the accessibility model. Principal barriers reported include non-inclusive criteria for accessing services (taking account both parenthood and disability), lack of knowledge about the services offered and the inadequacy of services in addressing parents’ needs. The sixth dimension (“offers and resistance”) presents a dynamic element, as it relates to the parents’ decision to use – or not – a service to which they are entitled. Using this model allowed for a pragmatic and systematic description of the obstacles encountered by parents, as well as the identification of needs and potential directions for action.
Download the PDF version to access the complete article, including figures and tables.
Background
In recent decades, more and more people with disabilities have become parents (Blackford et al., 2000; Office des personnes handicapées du Québec [OPHQ], 2009). This can be explained by the advancement of medical technology, but also by major changes – in the context of Quebec province – in the paradigms concerning people with disabilities, with a focus on strengthening their full social and civic participation (E-20.1 - Act to secure handicapped persons in the exercise of their rights with a view to achieving social, school and workplace integration, 1978; United Nations, 2006). For example, in the province of Quebec (Canada), the establishment of the Office des personnes handicapées du Québec – an office dedicated to forwarding the rights and civic participation of people with disabilities – and one of its policies from 2009 (OPHQ, 2009) are actively supporting the full social participation of persons with disabilities, including the right to embrace a parental role (although this is not explicitly detailed in the policy referenced). Despite the shift in the perception of disability in Quebec, there are still marked differences between people with and without disabilities in terms of family life. Indeed, people with disabilities aged 15 to 64 years are more likely to live alone (27.2%) than people without disabilities (11.6%) (Camirand, 2010). They are also less likely to be married or in a common-law relationship: 54% versus 62% of the non-disabled population (OPHQ, 2017). There is also still "persistent and systemic" discrimination against them when it comes to parenting (National Council on Disability, 2012).
In the field of perinatal and early childhood in Quebec (Canada), various medical and psychosocial services and follow-ups are offered to all parents, universally, to support them at different stages of their experience, including pregnancy, childbirth, and infant care (Institut national de santé publique du Québec, n. d) : pregnancy follow-ups, discussions of a birth plan, breastfeeding support, for instance. These kind of services are valuable resources for parents in preparing for their new role as well as in supporting them as parents (Delawarde et al., 2014). Easy access to the services in question is an important prerequisite for promoting positive health outcomes – physical and mental health – for both parent and child (Lawler et al., 2013; Mitra et al., 2015). Conversely, barriers in access to services can lead to problems on three levels: 1) service utilization, 2) patient (parent) satisfaction, and 3) inadequate professional practices (Lawler et al., 2013). Therefore, we might think that facilitating accessibility to services is a major step in promoting equitable care.
However, existing literature highlights that, despite the increase in the number of parents with physical disabilities, their access to perinatal and early childhood services (usually services offered when the child is between 0 and 5 years old, depending on the programs) remains impeded at several levels. First, various studies mention significant gaps in the availability of information about the existence of services (Begley et al., 2009; Lawler et al., 2013; Tarasoff, 2015, 2017). Second, the literature indicates that access to services is impeded, partially due to:
More specifically, physical access is hindered on two levels: 1) access to the buildings within which the service is provided (Begley et al., 2009; Bergeron et al., 2012; Lawler et al., 2013) and 2) access to pregnancy monitoring equipment or hospital facilities (particularly delivery rooms) (Becker et al., 1997; Mitra et al., 2016, 2017). For example, several studies (Iezzoni et al., 2015; Mitra et al., 2016) have shown that some women with physical disabilities did not have access to a complete pregnancy follow-up due to a lack of appropriate equipment (for example, adapted scales or examination tables). These results highlight a major obstacle in pregnancy follow-up that could ultimately be harmful to the health of the baby and the mother. On a related front, the organization of services in silos – having services specialized only in the field of perinatality/parenthood and services specialized only in the field of disability – could also be seen as a barrier to the well-being of parents with physical disabilities, who need to be taken care of in a more integrated bio-psycho-social framework of care (Grue & Lærum, 2002; Mitra et al., 2015). For example, as for services specialized only for people with disabilities, the Quebec government offers home support services to support them with their activities of daily living (hygiene, household chores), as well as adapted transportation services.
The concept of access is a complex one and its definition is not unanimously agreed upon in the scientific literature (Penchansky & Thomas, 1981; Ricketts & Goldsmith, 2005). For the purpose of this article, we will be using the Dixon-Woods et al.’ model (Dixon-Woods et al., 2006), from their review of the literature on access to health services for socio-economically disadvantaged people (Dixon-Woods et al., 2006). This model is pertinent, as it presents a dynamic definition of access, with an emphasis on the following two characteristics: 1) access to, and eligibility for a service is a negotiation between the individual and the service itself ; 2) access to a service can be conceptualized temporally, where the dimensions of Dixon-Woods et al. (Dixon-Woods et al., 2006) can be seen as chronological stages through which individuals must pass (one must first recognize one's need and be able to get to the service before confronting it, claiming it, and dealing with possible professional judgements). This model is composed of six dimensions:
The objective of this article is to analyse, through the accessibility model of Dixon-Woods et al. (Dixon-Woods et al., 2006), barriers to access to perinatal and early childhood (0-5 years old) services, from the perspective of parents with physical disabilities. The data presented in this paper were part of a larger study about the experiences and needs of parents with physical disabilities with respect to their relationship with perinatal and early childhood services, the results of which are presented in a prior article (Mercerat & Saïas, 2020). This study focused exclusively on parents with physical disabilities. This choice was made in collaboration with an advisory comity working on the general study and was also supported by the fact that physical disabilities represent the most common disabilities found in the general Canadian and Quebec population. In Quebec and across all age groups, the number of people with disabilities related to mobility (8.5%), agility (8.2%) or pain (7.8%) surpasses the number of people with other types of disabilities (Camirand et al., 2010). In addition, a review of the literature shows that people with physical disabilities have been less represented in parenting studies in recent years (vs. people with intellectual and developmental disabilities, for instance). The notion of "barriers" refers to any difficulties shared by the parents participating in this study related to their access to services. The “perinatal and early childhood services” are understood as services offered throughout parenthood, from the decision to have a child (prenatal), until the child is approximatively 5 years old (postnatal). The term “services” in an intentionally broad term, as we wanted to allow participants to choose which services surrounding their parenthood they wanted to discuss, and which services were the most significant for them in their parenting role.
Finally, this paper aims to address the complexity of the notion of accessibility, which is not a dichotomous “on/off” concept, but rather a dynamic, multi-dimensional concept.
Methods
A qualitative methodology based on the life story approach (Bertaux & de Singly, 2005; Burrick, 2010; Sanséau, 2005) was selected for the study. Indeed, as the transition to parenthood can have a profound impact on a person’s identity (Poissant et al., 2014) and can be understood using a temporal perspective, the choice of a life story approach allowed participants to insert parental events, within the context of their broader life experiences (and therefore their experience as persons with disabilities).
In-depth individual interviews were conducted with parents – mothers and fathers – with various physical disabilities. The interviews were designed to last between 60 and 90 minutes. Interviews were either conducted in person or by phone/videocall. Recruitment was carried out with the help of a specialized resource for parents with physical disabilities (a service provided by occupational therapists specifically to parents with physical disabilities, offered in the health and social services system) and through community disability rights organizations. The parents interviewed for this study had to meet the following inclusion criteria:
Parents who could not complete an interview in French or who had significant intellectual or sensory impairments – as self-assessed – were excluded from the sample.
At the outset of each interview, participants were asked to sign a consent form, as approved by a research ethics board (CRIR : certificate #1216-0217 delivered on April 25th 2017). Participants were also provided a sociodemographic questionnaire to complete, which included questions regarding age, education, marital status, and number of children.
In the interview, they were invited to talk about their lives in general terms ("can you talk to me about your general life experience, starting when or where you decide, for example, from your birth or your diagnosis? "), and then more specifically about their parenting experience. Referring to this experience, the interviewer asked participants to elaborate on the services they had received in relation to their parenting role. More in-depth questions followed, exploring their needs and how the services accommodated them, as exemplified in the following table.
Table 1. Research sub-questions based on the six dimensions of Dixon-Woods et al. (Dixon-Woods et al., 2006) (Download the PDF version to access the complete article, including figures and tables.)
All interviews were audio-recorded and transcribed verbatim. To ensure the anonymity of the participants, all names or places that could identify the study participants have been removed. Pseudonyms were also assigned to participants in order to report and disseminate results while protecting their confidentiality.
For data analysis, all interviews were coded using QSR International’s NVivo 12 software, following the six steps of thematic analysis recommended by Braun and Clarke (Braun & Clarke, 2006) : 1) familiarizing with the data; 2) generating initial codes; 3) searching for themes; 4) refining the themes; 5) defining and naming the themes; and 6) producing the data report. The relevance of Braun and Clarke's process-based analysis (Braun & Clarke, 2006) lies in the fact that this method is highly flexible and is well suited to the analysis of data obtained using the life story method (Braun & Clarke, 2006). The systematic nature of such a method of analysis also makes it reliable for producing qualitative analysis that can inform and support the development of public policy (Braun & Clarke, 2006). To ensure reliability in the data analysis process and to obtain inter-evaluator agreement, the two authors worked collaboratively on coding the first three interviews. Once the general coding grid defined, the first author coded the remaining interviews.
The analysis for this specific paper concentrated specifically on the narrative description of access to services, previously coded with Braun and Clarke’s method (Braun & Clarke, 2006). For this specific part of the data, a pre-analysis grid was defined, consisting of the six dimensions of Dixon-Woods et al. (Dixon-Woods et al., 2006) presented above. The authors, while following the participants’ narratives as closely as possible, classified the parts of the narratives previously coded as relating to access to services into these different dimensions.
Sample characteristics
The sample in the study consisted of thirteen parents, including 10 mothers and 3 fathers, with various physical disabilities: amputation (n=1), rheumatoid arthritis (juvenile) (n=2), arthrogryposis (n=1), chronic pain (n=1), degenerative neuromuscular disease (for example, multiple sclerosis) (n=3), cerebral palsy (n=2), spina bifida (n=1), tetraplegia or partial paralysis (n=2). The majority of parents were in the 30–39 age group (n=11), while the remainder were aged 40–49 (n=2). Most participants had a university degree, either undergraduate (n=6) or graduate (n=2). The remainder had either a high school (n=1) or college (n=3) education. In terms of their family situation, two participants were separated or divorced, four were living with a common-law partner – which is common in Quebec – and seven were married. Finally, the number of children per participant varied. Five participants reported having only one child, four participants had two children, three participants had three children, and only one participant reported having four children.
Interviews were conducted in participants’ homes or by videoconference between July 2017 and March 2018. Interviews ranged in length from 30 minutes to two hours. The number of participants was determined based on the principle of data saturation (Savoie-Zajc, 2007), meaning that as less new information began to emerge from the interviews, participant recruitment was stopped.
The results are presented in the following section, according to the dimensions of the Dixon-Woods et al. (Dixon-Woods et al., 2006) model, along with supporting excerpts that have been translated from French. As interviews took place in French, a professional translator was in charge of the translation of the quotations presented in this paper. All quotations are provided verbatim from interviews.
Results
Presentation of the results following Dixon-Woods et al. accessibility model
Identification of candidacy
The “identification of candidacy” dimension has two elements: (1) participants’ perception of their eligibility for a service; and (2) their sense that the service can meet their needs. In the interviews, the factors influencing these elements, as reported by parents, relate to the admissibility/eligibility criteria for the services in question.
In this regard, the lack of consideration for parenting within services directed at people with disabilities was frequently discussed. Several parents reported a lack of support for their right to become, or to be, a parent when they were requesting services (for example, home support hours), even though they themselves considered themselves eligible for the service. In the following excerpts, Paul talks about his perception of his own eligibility in his request to obtain more hours of home support (home support services – household chores) and Laura about the lack of adapted equipment to take care of her baby and her feeling of being ‘outside the boxes’.
Based on the law on equality and rights, you have the right to be a parent, but... it’s a right that isn’t supported [by the services already in place]. (Paul, living with cerebral palsy)
The thing is, if you step outside of the norm or the usual framework, then there’s nothing there. You just fall into the gap. (Laura, living with arthrogryposis)
In similar contexts, some parents were told that they did not meet criteria for receiving services, due to their level of income (too high) or the lack of consideration of parenthood in the context of disability among the selection criteria for certain services:
I was also told that I didn’t fit the criteria because I had a high salary, supposedly I could have afforded whomever I wanted. (Mila, living with rheumatoid arthritis)
From this discussion, an important theme was raised: the services offered to people with disabilities are often not adapted to their reality as parents. The next two dimensions of the model – navigation and permeability – highlight an ‘inverse’ but intrinsically related problem, namely, that so-called ‘universal’ perinatal and early childhood services sometimes fail to take parents’ physical disability into account.
Navigation
Navigation refers to the ability to know what services are available and to be able to get to those services, especially concerning physical travel. Navigation refers to the knowledge of the participants (parents) and of the professionals related to pertinent services. Issues related to professionals’ knowledge of services and to physical access to services came up repeatedly in the participants’ comments.
In this regard, medical staff’s lack of knowledge about programs specifically geared to parents with physical disabilities were mentioned. For example, physicians responsible for pregnancy monitoring would not spontaneously propose specialized services that could meet parents’ needs (for example services providing adapted equipment to take care of the child). In this regard, one participant emphasized that, in her opinion, it should be the physicians’ responsibility to be aware of appropriate and beneficial resources:
If you don’t have resources to begin with, and no one tells you about them, you may miss out on something. I think that doctors do have a responsibility to at least know what the resource is. (Elisabeth, living with partial paralysis)
This same participant also reported that she felt obliged to take the initiative to find out about the service she needed, at the risk of missing out on an advantageous resource.
These observations were consistent with other statements by parents who reported not being aware of services that would meet specific needs related to their physical condition, as in the case of Emily, a mother living with spina bifida:
I know that the service itself [a service for parents with additional needs], […] I don’t think it’s there.
The above results highlight the parents’ need to be better supported in finding services that meet their reality. According to the parents in this study, professionals seem to have an important role to play in this support, particularly through their knowledge of the health and social services system.
Regarding the participants’ ability to physically attend known services, several mothers in the sample noted that maternity wards and examination rooms – particularly with regards to the furniture – were not suitable for them. Other mothers complained that prenatal classes or postnatal mother-baby activities were held in locations that were not physically accessible, experienced by Victoria:
What I actually missed during my maternity leave was… doing social mom activities … being able to go out, do workshops on baby stuff. Most of the places weren’t accessible. (Victoria, living with a degenerative neuromuscular disorder)
Permeability of services
Permeability refers to how the parent perceives the ability of the service to adapt to their needs. On this front, a lack of flexibility or a rigidity in the provision of the services received were reported, which sometimes hindered the assistance being provided. In the following excerpt, Kate – a mother living with cerebral palsy – shares her experience with paratransit transportation and its rigidity when it comes to transporting her children:
Technically, officially, paratransit, they don’t want to be responsible for taking the car seat, installing it, … you know. So they just said to me, in about as many words, “Well, your daughter, you can bring her, because she can carry her [car seat] by herself, but your little boy, as long as he’s in a big car seat, Stage 2, well... we’d much rather that... you don’t bring him.”
It was also noted that some professionals practicing in perinatal services were not able to accommodate parents’ needs. For example, Alice, a mother living with chronic pain, reported that she did not receive enough help from the local health centre to support her with day care services. This mother did not have a place for her daughter in a day care facility close to her home and the fact that she was living with physical limitations was not taken into account by the service in question. Alice shared that no one could help her with this situation. Other participants complained about inflexibility on the part of the professionals responsible for their cases, as described below by Laura, a mother living with arthrogryposis:
People build frameworks to have some form of structure, but... every individual is different.
The occupational therapist who was on my case, because she decided not to fight against their structure, to keep her distance and accept the norm, well she felt really disappointed, not being able to help me.
The above excerpts thus refer to the needs of parents with physical disabilities for parenting and disability services to be more intersectional, in order to best respond to their realities.
Appearance at health services
Different elements of the participants’ narratives related to feeling unwelcome or overlooked when trying to access services. In this regard, difficulties in obtaining the service needed or in following up once the service had been requested were highlighted. Some parents mentioned inadequacies in some of the services they received – such as home care support – or the possibility that services would be suspended due to budget cuts. Paul, a father living with cerebral palsy, even reported feeling “betrayed by the system” as a result of service cuts.
In this context, Paul and Alice mentioned that they have had to fight to obtain the services to which they thought they were entitled, as stated in the following citations:
Today, I had to fight. Hard. [Laughs] ... To get the same thing [as in the first pregnancy] Because budgets … have been cut. (Paul, living with cerebral palsy)
You know, I don’t want to be treated differently, I don’t necessarily want what I’m not entitled to. But I think there are things ... that should have been done in my case, that were not done. Did I take everything for granted? No. You know, I knew it wasn’t going to be easy, I knew that all the battles weren’t ... going to be won in advance and all that, but you know I didn’t think I would have to do… to prove some things you know? (Alice, living with chronic pain)
Laura noted that she had to be assertive in declaring her wishes regarding how her general anaesthesia would be managed, in an attempt to regain control over her delivery:
And then I asked to meet the anaesthetist. I told her the story [of her first pregnancy]. I told her... how I would like it to happen. I checked with her to see if it could be done that way [to be woken up soon after the general anaesthesia], she said, “No worries.” (Laura, living with arthrogryposis)
In some instances, parents noted that they were denied services (for example hours for home support with household chores), for a variety of reasons, including the fact that the participant was employed or that the service requested was not directly related to parenting (e.g., home adaptations), even though such services would have helped in the parenting role (for example by allowing them to navigate their home easily in order to attend to their children at night). Faced with this lack of assistance, some parents reported that they had to make up for the lack of services financially, for example by purchasing adapted equipment themselves, paying directly for the necessary services, or accessing private health services.
Adjudications
‘Adjudications’ refer to professionals’ perceptions and/or judgments regarding parents’ access to the service. This dimension reinforces the idea that the accessibility of a service is a negotiation between the person - seeking for the service - and the service itself, including the professionals who work there. Parents reported various concerns relating to judgments or decisions made by professionals (health and social professionals) that impacted their subsequent progression through services. Some parents brought up remarks or judgements made by professionals, for example in relation to their desire of becoming parents. In this respect, one mother reported an instance in which medical residents doubted her parental ability, leading them to consider calling child protection services:
They [the residents] asked me if... they should call the DYP [child protection service] to take care of my children or... help me with this because they thought I couldn’t take care of them on my own. [...] I was very upset because she was my second daughter, so ... for me it’s ... I didn’t understand the reasoning. (Sophie, quadriplegic)
In connection with this same event, Sophie questioned why disabled parents are often treated differently than non-disabled parents:
They didn’t call the DYP or anything, but... at the time... you wonder why [they asked], because... I don’t think people who don’t have disabilities get asked that from the outset
Offers and resistance
On some occasions, despite services being offered, parents did not accept them. In some cases, the parents reported having discharged the professional who was doing their follow-up (for example the medical team or the occupational therapist). The following excerpts highlight the reasons that might have prompted parents to terminate their relationship with professionals. Some of these reasons are tied to other dimensions of the model, especially permeability of services and adjudications.
She [the midwife] was also another case of framework-thinking, [...] she says, “Since you had a caesarean section for the first baby, you can’t deliver at home.” So, for them, that’s their rule, so that’s the way it is. So ... I let my midwife go, finally, saying: “I feel strong enough to be home alone to give birth.” (Laura, living with arthrogryposis)
It’s all... it’s little things and then I was frustrated because she [an occupational therapist] wouldn’t listen. And so, I said to her, “You’re making my experience really unpleasant. Really, really, really unpleasant. In fact, I don’t even want your help.” (Lisa, living with juvenile rheumatoid arthritis)
In other instances, parents opted not to ask for help or services, even when they were available.
Discussion
The purpose of this article was to analyse barriers to access to perinatal and early childhood services from the perspective of parents with physical disabilities. To this end, the six dimensions of Dixon-Woods et al. (2006) served as a framework for creating a data analysis grid specifically for the parts of a greater data corpus related to access to services. Since the term ‘services’ was not defined for the participants, the results allowed us to address a very broad understanding of ‘services surrounding parenting’ in the parents’ interviews. Indeed, on various occasions parents identified barriers to accessing services that one might not have easily identified as being related to their parenting role at first glance – for example, paratransit or home adaptation services. This finding highlights the fact that services that are seemingly removed from the parental role can undoubtedly enhance the well-being and sense of daily self-efficacy of parents with physical disabilities and help them feel more independent in their parenting role. Regarding the more “typical” services targeting the perinatal period and early parenthood, parents outlined several barriers that have also been discussed in other studies, such as staff’s lack of knowledge (Lipson & Rogers, 2000; Long-Bellil et al., 2017; Mitra et al., 2016; Schildberger et al., 2017; Smeltzer et al., 2017; Walsh-Gallagher et al., 2012), lack of physically adapted rooms, for example in maternity wards (Iezzoni et al., 2015; Mitra et al., 2017; Tarasoff, 2017; Thomas & Curtis, 1997) and judgmental attitudes of professionals (Blackford et al., 2000; Lipson & Rogers, 2000; Mitra et al., 2017; Payne et al., 2014; Smeltzer et al., 2017; Tarasoff, 2017). Parents were also repeatedly disappointed by the lack of consideration for their parental status in the evaluation of their case by medical and psychosocial managers. These observations are consistent with other research that already highlights the ‘silo’ management of individuals with multiple concurrent needs, particularly in the areas of disability and parenting (Grue & Lærum, 2002; Mitra et al., 2015). This observation points to a possible distinction between the experience of an inadequate system (where services simply do not exist) and unresponsive or insufficient implementation of services at the intersection of parenting and disability supports. This study allowed us to highlight that both of these scenarios were at play in the current health and social services system: either services targeting parents with physical disabilities do not exist (with the exception of one in the Province of Quebec, to our knowledge), or services are available, but the needs assessment grids for parents (in the general population) or for people with physical disabilities (not necessarily parents yet) do not intersect.
The results of this study underlined two principal domains where parents are particularly engaged in their access to perinatal and early childhood services : 1) their assertiveness in negotiating access to services designed to meet their needs (which refers to the five first dimensions on the Dixon-Woods et al.’s model), and 2) their choice to engage – or not – in the appropriate service (which relates to the last dimension – offers and resistance – of the model).
Being assertive and entering the negotiation
The results of this study revealed access barriers in all dimensions of the model. In this regard, the first five dimensions of the Dixon-Woods et al. (Dixon-Woods et al., 2006) model remain relatively descriptive and are related specifically to the process of negotiation between the parent and the service: does the parents recognize themselves as eligible for a given service? Are they aware of the service? Are they able to get there? Can the service be adapted to their needs? Do they feel judged by the professional? The model remains relevant for describing in a pragmatic and systematic way the access barriers encountered at all stages of accessing a service. The different dimensions of Dixon-Woods et al. were initially a product of a literature review on socioeconomically disadvantaged people (Dixon-Woods et al., 2006). However, such a model is relevant for parents with physical disabilities, as they can be seen as "vulnerable" (e.g. facing multiple challenges), and therefore, the model provides a useful construct for analysing the participants' negotiation with the services. The idea of "negotiation" was particularly evident in the participants' interviews, when they discussed situations in which they had to advocate for their rights to parenthood and accessing services. In some cases, parents also struggled to obtain or maintain service access (e.g., Paul, a father with cerebral palsy, who struggled to maintain the number of hours of home support during his wife's pregnancy), in the context of social and health services that were under financial stress due to budget cuts in Quebec.
The experiences of parents with disabilities who at times were advised by medical professionals to avoid parenthood (Walsh-Gallagher et al., 2012) and who lacked information about the impact of their disability on pregnancy (Mitra et al., 2016, 2017; Smeltzer et al., 2017) are highlighted through the dimensions of Dixon-Woods et al. (Dixon-Woods et al., 2006). These observations can be characterized by the navigation dimension (participants described a lack of knowledge – on their part and on the part of professionals – about the existence of services as well as difficulties in physically accessing them), the permeability of services dimension (according to the participants, several services did not take into account both their parental role and their disability), and the appearance at services dimension (several parents mentioned that they had to be assertive in order to convey their needs and possibly receive services). The reactions of professionals – including some judgments – are also obstacles that parents must deal with as they navigate life in their new social role.
Engaging – or not – in appropriate services
As in previous scientific literature, the parents reported barriers related to lack of knowledge about the existence of services, lack of physical accessibility of services, and lack of adaptation of services to meet their needs (Thomas & Curtis, 1997). This last point seems to be particularly significant with respect to parents’ decision to use – or not to use – an offered service. While the five first dimensions of the model were more descriptive in nature, the last dimension reflects a more dynamic process, recognizing the parent’s power and ability to choose, whether it is a real choice or a non-choice (a default choice). In the Dixon-Woods et al.’s model, although the five first dimensions referred specifically to the notion of negotiation between parents and services, the last dimension is the final step following the negotiation: does the parent choose to engage in the service or not? Considering our findings, it is important to note that parents sometimes chose not to engage in services that were intended for them, but which could – in their view – reinforce inequalities or discrimination against them. However, from the perspective of universality of care, this latter dimension may also reflect blatant inequality, making the parents responsible for their own care and for complying with what is expected of them in order to receive a service. This last dimension remains as a question to be explored further in future research, to determine whether alternative care channels might be more beneficial for parents with physical disabilities.
Our results should be understood with consideration of the limitations that existed in this study. First, the sample of participants does not appear to be representative of the ‘general’ population of persons with disabilities, with a disproportionate number of participants being in couples and having a university education, for example. While seeking ‘representativity’ of a sample is not central to qualitative research (Yardley, 2000, 2008), the fact that the majority of participants were married or in a relationship, and had a high level of education may give a more ‘privileged’ perspective of the experiences of parents with physical disabilities. Overall, though, it is difficult to conclude whether our sample was representative of the population of parents with disabilities, as we do not have any precise statistics on this subject. Second, it appears that the parents we interviewed were more inclined to share obstacles and dissatisfactions regarding the services they encountered, even when this portrayal was not wholly representative of their overall experience. Indeed, in a prior, more general study, parents did report positive and satisfying experiences with perinatal services (Mercerat & Saïas, 2020). However, most results still fell mainly on the negative or unsatisfied side, which led us to frame this article around barriers to access. In this sense, future research can take a more positive approach, with the aim of identifying interventions that could be implemented at various stages to promote service accessibility. Finally, interviewing some participants in person, while interviewing others over video-call, as well as the discrepancies between the lengths of the interviews (from 30 min to 120 min) are also limitations of this study. This is because the length of the interview can impact the depth of the information shared by the participants and doing interviews by video-call – in contrast to face-to-face interviews – may impair the relationship between the participant and the researcher.
Conclusion
Results of this study highlighted challenges in accessing perinatal and early childhood services for parents with physical disabilities. This article emphasizes the immediate importance of improving the accessibility of perinatal and early childhood services and adapting these services to meet the needs of parents with physical disabilities. Strengthening access to high-quality, adapted services is expected to have various positive impacts on maternal and child health, family well-being, quality of life within the family, and prevention of child abuse and neglect. The lessons we can draw from this study, for the practice of community psychology, are that parents with additional needs (in this case, related to their physical disabilities) do not receive the universal perinatal and early childhood services to which they are entitled, and continue to receive judgment from professionals regarding their parenting role. As community psychologists, one of our areas of intervention is the reduction of social inequalities in health, notably by promoting access to health services. In this context, our role is to use our tools (analytical skills, knowledge production) to promote equal access for all, by 1) strengthening a positive relationship between health institutions - including the professionals who work in them - and service users, and 2) exposing the power dynamics at play. Now that we have a better understanding of the barriers to accessible parenting services for parents with physical disabilities, future research should explore the actions that must be taken – or that parents are already taking, as some mentioned in interviews – to overcome these barriers.
References
Becker, H., Stuifbergen, A., & Tinkle, M. (1997). Reproductive health care experiences of women with physical disabilities: A qualitative study. Archives of Physical Medicine and Rehabilitation, 78(12, Supplement 5), S26–S33. https://doi.org/10.1016/S0003-9993(97)90218-5
Begley, C., Higgins, A., Lalor, J., Sheerin, F., Alexander, J., Nicholl, H., Lawler, D., Keenan, P., Tuohy, T., & Kavanagh, R. (2009). Women with Disabilities: Barriers and Facilitators to Accessing Services During Pregnancy, Childbirth and Early Motherhood (p. 215). School of Nursing and Midwifery, Trinity College.
Bergeron, C., Vincent, C., & Boucher, N. (2012). Experience of parents in wheelchairs with children aged 6 to 12. Technology and Disability, 24, 247–261. https://doi.org/10.3233/TAD-120356
Bertaux, D., & de Singly, F. de. (2005). L’enquête et ses méthodes: Le récit de vie (2e éd..). Armand Colin.
Bertschy, S., Geyh, S., Pannek, J., & Meyer, T. (2015). Perceived needs and experiences with healthcare services of women with spinal cord injury during pregnancy and childbirth—A qualitative content analysis of focus groups and individual interviews. BMC Health Services Research, 15(1), 234. https://doi.org/10.1186/s12913-015-0878-0
Blackford, K. A., Richardson, H., & Grieve, S. (2000). Prenatal education for mothers with disabilities. Journal of Advanced Nursing, 32(4), 898–904. https://doi.org/10.1046/j.1365-2648.2000.t01-1-01554.x
Boisseau, B., Perrouin-Verbe, B., Le Guillanton, N., Derrendinger, I., Riteau, A.-S., Idiard-Chamois, B., & Winer, N. (2016). Grossesse chez les femmes blessées médullaires: État des connaissances. Journal de Gynécologie Obstétrique et Biologie de La Reproduction, 45(9), 1179–1185. https://doi.org/10.1016/j.jgyn.2016.08.017
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. http://dx.doi.org/10.1191/1478088706qp063oa
Burrick, D. (2010). Une épistémologie du récit de vie. Recherches Qualitatives, Hors-Série(8), 7–36.
Camirand, J. (2010). Prévalence de l’incapacité dans la population québécoise. In Vivre avec une incapacité au Québec: Un portrait statistique à partir de l’Enquête sur la participation et les limitations d’activités de 2001 et 2006 (Institut de la statistique Québec, pp. 55–78).
Candilis-Huisman, D., Dommergues, M., Becerra, L., & Viaux-Savelon, S. (2017). Handicap moteur, maladies rares et maternalité: Une revue de la littérature. Devenir, Vol. 29(4), 307–325.
Delawarde, C., Briffault, X., Usubelli, L., & Saïas, T. (2014). Aider les parents à être parents ? Modèles et pratiques des programmes « evidence-based » d’aide à la parentalité. Annales Médico-Psychologiques, Revue Psychiatrique, 172(4), 273–279. https://doi.org/10.1016/j.amp.2012.12.007
Dixon-Woods, M., Cavers, D., Agarwal, S., Annandale, E., Arthur, A., Harvey, J., Hsu, R., Katbamna, S., Olsen, R., Smith, L., Riley, R., & Sutton, A. J. (2006). Conducting a critical interpretive synthesis of the literature on access to healthcare by vulnerable groups. BMC Medical Research Methodology, 6(1), 35. https://doi.org/10.1186/1471-2288-6-35
E-20.1— Act to secure handicapped persons in the exercise of their rights with a view to achieving social, school and workplace integration (1978).
Grue, L., & Lærum, K. T. (2002). “Doing Motherhood”: Some experiences of mothers with physical disabilities. Disability & Society, 17(6), 671–683. https://doi.org/10.1080/0968759022000010443
Iezzoni, L. I., Wint, A. J., Smeltzer, S. C., & Ecker, J. L. (2015). Physical Accessibility of Routine Prenatal Care for Women with Mobility Disability. Journal of Women’s Health, 24(12), 1006–1012. https://doi.org/10.1089/jwh.2015.5385
Institut national de santé publique du Québec. (n. d.). Périnatalité et petite enfance. Retrieved the August 11, 2020, from https://www.inspq.qc.ca/perinatalite-et- petite-enfance
Kelley, S. D. M., Sikka, A., & Venkatesan, S. (1997). A review of research on parental disability: Implications for research and counseling practice. Rehabilitation Counseling Bulletin, 41(2), 105–121.
Killoran, C. (1994). Women with disabilities having children: It’s our right too. Sexuality and Disability, 12(2), 121–126. https://doi.org/10.1007/BF02547886
Lawler, D., Lalor, J., & Begley, C. (2013). Access to Maternity Services for Women With a Physical Disability: A Systematic Review of the Literature. International Journal of Childbirth, 3(4), 203–217. https://doi.org/10.1891/2156-5287.3.4.203
Lipson, J. G., & Rogers, J. G. (2000). Pregnancy, Birth, and Disability: Women’s Health Care Experiences. Health Care for Women International, 21(1), 11–26. https://doi.org/10.1080/073993300245375
Long-Bellil, L., Mitra, M., Iezzoni, L. I., Smeltzer, S. C., & Smith, L. D. (2017). Experiences and unmet needs of women with physical disabilities for pain relief during labor and delivery. Disability and Health Journal, 10(3), 440–444. https://doi.org/10.1016/j.dhjo.2017.02.007
Mercerat, C., & Saïas, T. (2020). Parents with physical disabilities and perinatal services: Defining parents’ needs and their access to services. Disability & Society, 0(0), 1–24. https://doi.org/10.1080/09687599.2020.1788513
Mitra, M., Akobirshoev, I., Moring, N. S., Long-Bellil, L., Smeltzer, S. C., Smith, L. D., & Iezzoni, L. I. (2017). Access to and Satisfaction with Prenatal Care Among Pregnant Women with Physical Disabilities: Findings from a National Survey. Journal of Women’s Health, 26(12), 1356–1363. https://doi.org/10.1089/jwh.2016.6297
Mitra, M., Long-Bellil, L. M., Iezzoni, L. I., Smeltzer, S. C., & Smith, L. D. (2016). Pregnancy among women with physical disabilities: Unmet needs and recommendations on navigating pregnancy. Disability and Health Journal, 9(3), 457–463. https://doi.org/10.1016/j.dhjo.2015.12.007
Mitra, M., Long-Bellil, L. M., Smeltzer, S. C., & Iezzoni, L. I. (2015). A perinatal health framework for women with physical disabilities. Disability and Health Journal, 8(4), 499–506. https://doi.org/10.1016/j.dhjo.2015.05.007
National Council on Disability. (2012). Rocking the Cradle: Ensuring the Rights of Parents with Disabilities and Their Children (p. 450). National Council on Disability.
Office des personnes handicapées du Québec. (2009). À part entière: Pour un véritable exercice du droit à l’égalité (p. 84). Office des personnes handicapées du Québec.
Office des personnes handicapées du Québec. (2017). Les personnes avec incapacités au Québec: Caractéristiques sociodémographiques et économiques. Volume 2 (p. 28). Office des personnes handicapées du Québec.
Payne, D. A., Guerin, B., Roy, D., Giddings, L., Farquhar, C., & McPherson, K. (2014). Taking It Into Account: Caring for Disabled Mothers During Pregnancy and Birth. International Journal of Childbirth, 4(4), 228–239. https://doi.org/10.1891/2156-5287.4.4.228
Penchansky, R., & Thomas, J. W. (1981). The Concept of Access: Definition and Relationship to Consumer Satisfaction. Medical Care, 19(2), 127–140. JSTOR.
Poissant, J., Chan, A., & Lévesque, S. (2014). Adaptation à la parentalité. Institut national de santé publique du Québec.
Prilleltensky, O. (2003). A Ramp to Motherhood: The Experiences of Mothers with Physical Disabilities. Sexuality and Disability, 21(1), 21–47. https://doi.org/10.1023/A:1023558808891
Ricketts, T. C., & Goldsmith, L. J. (2005). Access in health services research: The battle of the frameworks. Nursing Outlook, 53(6), 274–280. https://doi.org/10.1016/j.outlook.2005.06.007
Sanséau, Y. (2005). Les récits de vie comme stratégie d’accès au réel en sciences de gestion: Pertinence, positionnement et perspectives d’analyse. Recherches Qualitatives, 25(2), 33–57.
Savoie-Zajc, L. (2007). Comment peut-on construire un échantillonnage scientifiquement valide? Recherches Qualitatives, Hors Série(5), 99–111.
Schildberger, B., Zenzmaier, C., & König-Bachmann, M. (2017). Experiences of Austrian mothers with mobility or sensory impairments during pregnancy, childbirth and the puerperium: A qualitative study. BMC Pregnancy and Childbirth, 17(1), 201. https://doi.org/10.1186/s12884-017-1388-3
Smeltzer, S. C., Wint, A. J., Ecker, J. L., & Iezzoni, L. I. (2017). Labor, delivery, and anesthesia experiences of women with physical disability. Birth, 44(4), 315–324. https://doi.org/10.1111/birt.12296
Tarasoff, L. A. (2015). Experiences of Women With Physical Disabilities During the Perinatal Period: A Review of the Literature and Recommendations to Improve Care. Health Care for Women International, 36(1), 88–107. https://doi.org/10.1080/07399332.2013.815756
Tarasoff, L. A. (2017). “We don’t know. We’ve never had anybody like you before”: Barriers to perinatal care for women with physical disabilities. Disability and Health Journal, 10(3), 426–433. https://doi.org/10.1016/j.dhjo.2017.03.017
Thomas, C., & Curtis, P. (1997). Having a baby: Some disabled women’s reproductive experiences. Midwifery, 13(4), 202–209. https://doi.org/10.1016/S0266-6138(97)80007-1
Walsh-Gallagher, D., Sinclair, M., & Mc Conkey, R. (2012). The ambiguity of disabled women’s experiences of pregnancy, childbirth and motherhood: A phenomenological understanding. Midwifery, 28(2), 156–162. https://doi.org/10.1016/j.midw.2011.01.003
United Nations. (2006). Convention relative aux droits des personnes handicapées et protocole facultatif. Retrieved from https://www.un.org/disabilities/documents/ convention/convoptprot-f.pdf
Yardley, L. (2000). Dilemmas in qualitative health research. Psychology & Health, 15(2), 215–228. https://doi.org/10.1080/08870440008400302
Yardley, L. (2008). Demonstrating Validity in Qualitative Psychology. In Qualitative Psychology: A Practical Guide to Research Methods (SAGE).
Acknowledgements
The authors would like to thank the disability rights organizations who participated in the advisory board of this study for their valuable support. We would also like to thank Rachel Goldfarb for the English language revision, Marion Picot for her precise transcription work and to the CRUJeF for their financial support. Finally, we would like to express our deep gratitude to the research participants who found the time and courage to open up to our questions.
Declaration of interests
No potential competing interest was reported by the authors.
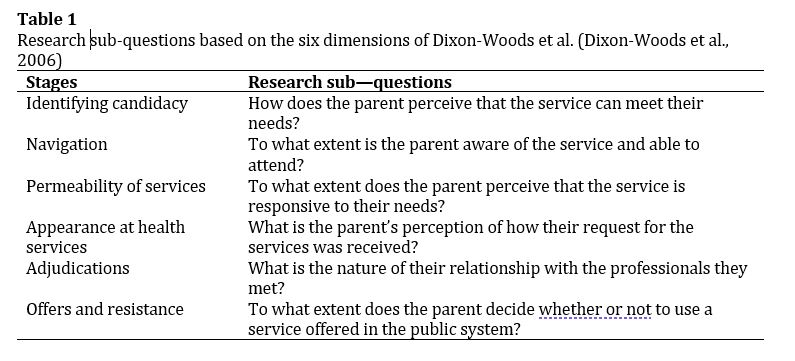 Table 1. Research sub-questions based on the six dimensions of Dixon-Woods et al. (Dixon-Woods et al., 2006) |
 Coralie Mercerat & Thomas Saïas
Coralie Mercerat & Thomas Saïas
Coralie Mercerat, is a Professor substitute in Psychology and Mental Health at the University TELUQ. Her work is about relationships between individuals (families) and health facilities, parenthood, reproductive justice and physical disability. She's also leading program evaluation projects with community organizations.
Thomas Saïas, is a Professor of Community Psychology at the University of Quebec in Montreal. He has been working in the field of early childhood prevention for the last 15 years. In France, he developed several public-orientated services of prevention (CAPEDP, PANJO, Petits pas Grands pas) which were the first interventions based on research ever led in the country. In Quebec and in France, he’s involved in several research projects aiming to identify the facilitators for the success of public (governmental) preventive interventions. He is currently head of the “Epione: public health-community health” research team.
Add Comment
![]() Download the PDF version to access the complete article.
Download the PDF version to access the complete article.
Keywords: parenthood, physical disabilities, accessibility, perinatal services, early childhood services.
 Based on a work at www.gjcpp.org.
Based on a work at www.gjcpp.org. 