Community health improvement initiatives are strongly influenced by the local context in which they take place. Community coalitions of diverse stakeholders are expected to determine the needs of their population of interest, select an appropriate strategy, implement with quality, and evaluate for effectiveness. Many public health initiatives look toward behavioral scientists with experience in collaborating with community members. The competencies that community psychologists possess make them particularly useful contributors in these initiatives, especially when the projects explicitly focus on increasing health equity.
This paper describes how community psychologists can contribute to community health improvement work by sharing our experiences in the Spreading Community Accelerators through Learning and Evaluation (SCALE) initiative funded by the Robert Wood Johnson Foundation. As part of SCALE, community coalitions are expected to develop appropriate aims and corresponding driver diagrams as well as implement quality improvement projects to help reach those aims. We demonstrate how community psychologists operationalize SCALE by working with communities of color in three distinct settings with different contextual factors: the Proviso Partners for Health (Chicago, IL), Boston Medical Center’s Vital Village Network (Boston, MA), and the San Gabriel Valley Healthy Cities Collaborative (Los Angeles, CA). We also describe how community psychologists contribute to the formative evaluation of the entire SCALE project. We note that specific community psychology competencies are applicable across diverse settings in community health improvement work. Consequently, community psychologists can contribute significantly to improving community health and advancing health equity.
Download PDF version for full article including all tables, figures, and appendices.
Introduction
Community psychologists work in a diverse range of settings and contexts. One emerging area for practice is community-based health improvement (Wallerstein & Duran, 2006; Campbell & Murry, 2004). Since community health improvement initiatives are strongly influenced by the local context in which they take place, they require both an in-depth understanding of the social and cultural factors that affect health outcomes and a commitment to working closely with local communities. As health organizations begin to shift toward implementing more population and community health models, there are great opportunities for community psychologists to contribute positively to this work. The core practice competencies of community psychology training and the professional identity of community psychologists are well aligned to meet the needs of community health improvement (Dalton & Wolfe, 2012).
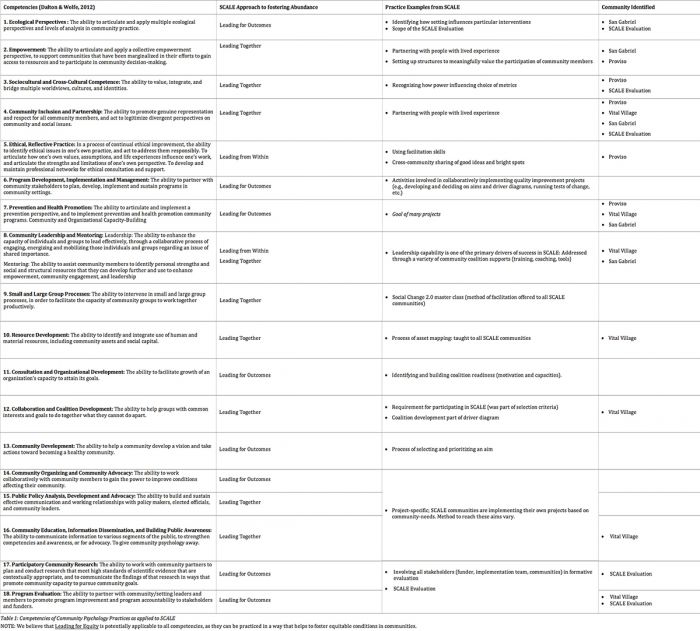
Traditionally, the public health field has incorporated knowledge from the social and behavioral sciences in order to enhance understanding of community-level health work (Green, 2008). Knowledge of social and ecological determinants of health is an area where community psychologists have expertise. Community psychologists integrate theory and action research and develop trusting long-term relationships with local community stakeholders. A focus on social justice, concretely operationalized by the core competencies of community psychologists, illustrates significant opportunities to engage the broader community on issues pertaining to health equity (see Table 1).
There is ample evidence that inequity negatively affects health outcomes, particularly in low-resourced communities (AHRQ, 2014). Working toward health equity for all is a major focus of many national policy initiatives (e.g. HHS, 2011; ASTHO, 2013). As an example, Healthy People 2020 defines health equity as the “attainment of the highest level of health for all people”. This simple definition belies the complex moral and practical challenges of how to effectively make decisions as a coalition and take action collaboratively that balance limited resources and promote fairness and justice for all, and doing so in situations when inequity is embedded in the structural and social systems of community health.
To achieve this requires the genuine inclusion of communities in the intervention development and delivery process (e.g., research, intervention implementation, and evaluation). Community psychologists are equipped to foster this type of community decision-making to help address the social determinants of health, and work toward promoting health equity in low-resourced communities. Community psychologists have the skills (Dalton & Wolfe, 2012) and the values/motivation (i.e., community psychology principles; SCRA, 2016; Kloos, Hill, Thomas, Wandersman, & Elias, 2011) to push for inclusion of multiple stakeholders and manage relationships among community members, researchers/academics, policy makers, and relevant others. Applying these skills in community health settings is a way to work toward reducing health disparities between different populations (Wallerstein & Duran, 2010) and improve overall wellness in communities.
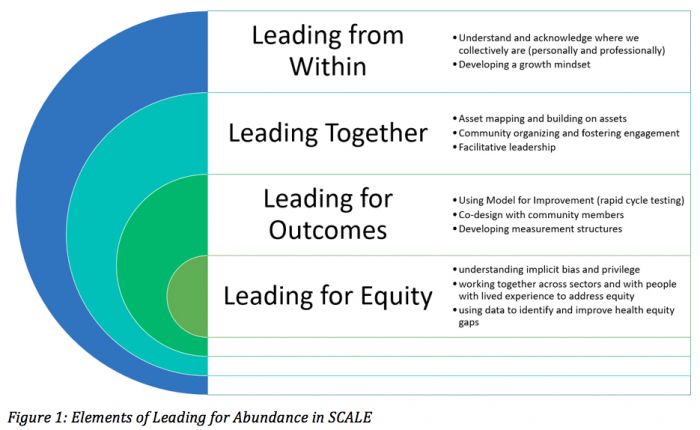
The Institute for Healthcare Improvement’s Spreading Community Accelerators through Learning and Evaluation (SCALE) initiative, funded by the Robert Wood Johnson Foundation (RWJF), has designed a unique approach to building equity for community health improvement that prioritizes trust and equitable relationships with meaningful implementation and evaluation (see Figure 1). Leading from within reflects the need for change agents to be consciously aware of one’s own identity in the social structure of society to promote equitable change. Leading together promotes the co-design processes that are central to community health improvement. This tenet guides the reality that the lived experience of community members and professional expertise are both needed to address the social determinants of health and promote equitable solutions. Leading for outcomes highlights the critical need for health improvement work to achieve meaningful systemic change using the tools of improvement science. Finally, Leading for equity explicitly calls out the need to maintain an equity-promoting mindset in all activities and applies the skills of leading from within (understanding one’s own bias), leading together (understanding the lived experience of inequity to create solutions whole growing the capacity of those most affected), leading for outcomes (using data to identify and improve equity gaps) to sustainably improve equity. Collectively, the SCALE leadership uses these frames to collective foster the skills of Leading for Abundance in communities.
Table 1: Competencies of Community Psychology Practices as applied to SCALE (See PDF version or JPG at the end of this article)
In this paper, we discuss how community psychology contributes to community health improvement by illustrating the core competencies in practice. We do this by sharing community psychologists’ unique experiences and insights stemming from their close collaboration with communities of color in three distinct settings within SCALE with different contextual factors: The Proviso Partners for Health (Chicago, IL), Boston Medical Center’s Vital Village Network (Boston, MA), and San Gabriel Valley Healthy Cities Collaborative (Los Angeles, CA). We also describe how community psychologists contribute to the formative evaluation of the entire SCALE project based on the insights and experiences of the evaluators who are community psychologists. In each of the sample cases we discuss, we describe how key community psychology competencies are applicable across diverse settings in community health improvement work and how the competencies are used to promote equity in communities of color.
Figure 1: Elements of Leading for Abundance in SCALE (See PDF version or JPG at the end of this article)
Project Setting
SCALE is led by the Institute for Healthcare Improvement (IHI) in collaboration with three partner organizations – Community Solutions, Communities Joined in Action, and the Collaborative Health Network. The SCALE initiative is designed in the spirit of Robert Wood Johnson Foundation’s (RWJF) vision to promote a culture of health for all by changing social, policy, financial, and community-level structures (Mockenhaupt & Woodrum, 2015). Broadly, SCALE is the first community-based program of the IHI-led global initiative, 100 Million Healthier Lives, which aims to achieve the goal of 100 million people living healthier lives by 2020 (IHI, 2016).
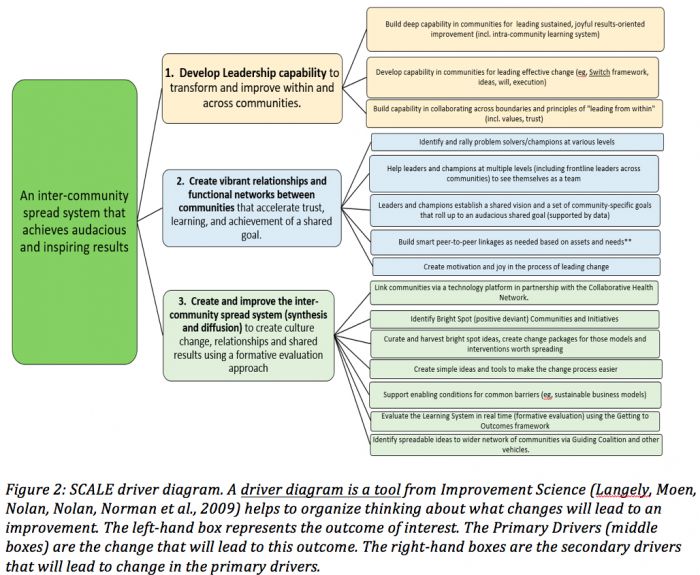
The overarching goal of SCALE is to increase the readiness and capability of communities to improve health, well-being and equity within communities. Working toward health equity is specifically called out as, “The price of admission” (IHI, 2016). To reach this goal, SCALE is targeting three primary drivers of change: 1) develop leadership capability to transform and improve within and across communities; 2) create vibrant relationships and functional networks between communities that accelerate trust, learning and achievement of a shared goal; and 3) create and improve the inter-community spread system. This full driver diagram can be found in Figure 2.
Figure 2: SCALE driver diagram. A driver diagram is a tool from Improvement Science (Langely, Moen, Nolan, Nolan, Norman et al., 2009) helps to organize thinking about what changes will lead to an improvement. The left-hand box represents the outcome of interest. The Primary Drivers (middle boxes) are the change that will lead to this outcome. The right-hand boxes are the secondary drivers that will lead to change in the primary drivers. (See PDF version or JPG at the end of this article)
Twenty-four community coalitions nationwide were selected through an application process that identified communities with experience in improving the health of their communities, and motivation to accelerate their work, to learn from others, and to contribute to a shared learning community. Selected community coalitions received funding over the 20-month period to support SCALE community health improvement efforts, travel to four immersive training events (Community Health Improvement Leadership Academies-CHILAs), and access to a variety of tools, supports and resources developed exclusively for the SCALE initiative.
As part of the selection process, community coalitions needed at least three partnering organizations representing different sectors (e.g., education, public health, social services, health care) who are working together to address the social determinants of health. This inclusion creates a challenge of operationalizing equity in collaboration. In such settings, community psychologists must be aware ofpower and resource differentials and assure these do not hurt relationships and trust among partners and especially that community members’ voices and decision-making is valued and respected. The promotion of equity in health and education in our communities and society begins within our own coalitions and collaborative partnerships.
In SCALE, one method to ensure this is by requiring that every coalition has a “Community Champion.” This is a person with lived experience (i.e. expertise that is not acquired through learning or training but through personal experience) who can use this knowledge to inform the development and implementation of community health improvement projects. Community Champions are an integral part of the coalitions and the process of including their voice and experiences is very intentional and thought out within SCALE. SCALE centrally supported champions by having special content and training dedicated to fostering their leadership skills. Many coalitions adopted a model of shared leadership on all levels (planning, implementation and now evaluation) and clearly communicated the role of champions to other institutional partners to guard against tokenism. Although SCALE leadership recommended that champions be compensated for their time because they may have challenges and barriers to participation, we do not have data on how consistently this was implemented across all SCALE communities.
The following sections will highlight four teams within the SCALE initiative. Each section below includes a short overview of our respective settings and projects. We will identify how community psychology competencies are utilized in each project. We will demonstrate how competencies are used to address health equity. The community-level projects for SCALE broadly fall under the community psychology competency of Prevention and Health Promotion. This is because many of the projects aim to improve the health, well-being, and equity within communities. The examples will demonstrate how community psychologists enact other competencies under the umbrella of prevention and promotion.
Each section was developed independently of one another. As a group, we did not specify which competencies we would address beforehand. Rather, we left it to the respective section author(s) to identify which competencies were most relevant to their work. We did decide, however, to make sure each of our sections address issues pertaining to Leading for Equity. We also note that, in many cases, examples apply to multiple competencies. When possible, we tried to preserve the voice of each author in these sections as they reflected upon their experiences in each of their projects. We parenthetically note the authors of each section. The Proviso Partners case focuses on power dynamics in decision-making in Leading from Within (SB, LH). The Vital Village Network case highlights the positive impact of working collaboratively for sustainability and Leading Together (KB). The San Gabriel Valley describes emerging learning on Leading Together and Leading for Outcomes (NC). Finally, the section on the SCALE Evaluation highlights how equity inform the types of methods and processes utilized (KA, JS).
Proviso Partners for Health
Proviso Partners for Health (PP4H) is a multi-sector coalition to support community health and economic development with a focus on school and community healthy food access and social entrepreneurship. The coalition serves four segregated African-American and Latino neighborhoods that experience disproportionate rates of obesity, unemployment, poverty, and low educational attainment. To address the complex challenge of these social and structural determinants of health, Proviso Partners promotes equity by sharing power and leadership, leveraging resources, and strengthening capacity of organizations and community members with lived experience. Currently, we are expanding our urban farm network and partnering with small urban agriculture businesses. The case description below describes how the community psychology competencies help to promote equity in the Proviso Partners coalition.
Collective impact initiatives represent diverse stakeholders working together to make changes around a common agenda with a group of staff that help to support the structure and facilitate an agreed-upon approach or group process (Kania & Kramer, 2011; 2013). As a multi-sector coalition engaged in various initiatives, it is valuable to explore the coalition processes, activities, and outcomes through the lens of community psychology. The core community psychology competencies provide a shared understanding of the group process, challenges, and potential for success in addressing chronic illness while promoting a health equity lens.
Sociocultural and Cross-cultural Competence
Sociocultural and cross-cultural competence in community psychology involves the “ability to value, integrate, and bridge multiple worldviews, cultures, and identities” (Dalton & Wolfe, 2012). PP4H explicitly aims to address sociocultural competence and health equity through our guiding principle of shared power and leadership. Despite our effective collaboration, there are complex social and cultural biases at play in our decision-making process (Kubota, Li, Bar-David, Banaji, & Phelps, 2013).
For example, partners faced the influence of racial and power status bias in a decision-making discussion on indicators for measurement. An African-American “novice” business owner introduced the outcome measure of community self-esteem as an important community level metric relevant to community members with lived experience. A white “experienced” business owner misinterpreted this suggestion as individual self-esteem. The group sided with the perspective of the experienced business owner and the importance of community level assessment was on the verge of being lost. Community self-esteem was dismissed as a concept once it was deemed irrelevant by the white “experienced” business owner. Using facilitation skills, a Community Champion and member of the leadership team used their influence and the SCALE training on communication to make everyone clear about the potential importance of community self-esteem as an outcome measure in our work. She explained that communities have identities and cultures that go beyond an assessment of a group of individuals. That critical moment highlights the skill of eliciting “open and honest communication,” which helps diverse partners engage in difficult conversations and not be influenced by the apparent racial and power dynamics in the conversation.
Community Inclusion and Partnership
Given the coalition’s focus on health, it was important to encourage co-design regarding health when community members interacted with faculty and staff from a local hospital and university. We intentionally did not want those from the university to be seen as “experts” on how to best address health outcomes and set the action plan for the community members. Currently, we strive to engage diverse community members (e.g. students, parents, teachers, residents, business owners, etc.) involved in the decision-making process. This involves community organizing and advocating for involvement at multiple levels and stages of the community change process, including organizational participation, leadership, program implementation, and evaluation.
Diverse community representation helps ensure that power, resources, and capacity are granted to those who have traditionally been disempowered and is part of our attempt to address health equity (Healthy People, 2020). Furthermore, the emphasis on inclusion with PP4H (and SCALE as a whole) helps to address one of Wolff’s (2016) central critiques of collective impact by meaningfully engaging community members who have been most affected by issues and consequently may possess unique knowledge about potential causes and solutions. For example, our executive leadership team, steering committee and work groups are each co-led by community members. One of the challenges of getting community members engaged has to do with life and work demands in their personal lives. Parents of young children can be difficult to reach because of the barriers of high unemployment in our community. Parents in communities of color can struggle to find high quality good paying jobs. For instance, a young mother lives in the west suburbs of Chicago, takes her children to childcare in the south suburbs, and works at a fast food restaurant in the north suburbs. This commute takes 2.5 hours by bus and train leaving limited time and energy for family and community health activities. We addressed this issue in PP4H by prioritizing funding an additional Community Champion as a critical priority of our SCALE process. It was important for us to pay our Community Champion in order to tap into their lived experiences and commitment to improving their community. Offering support for the time and energy of Community Champions involved in our project was one way we met the challenge of community engagement.
Ultimately, our coalition values the time, energy and voice of our community members and so we have decided that it is important to respect their willingness and commitment to improving their community. One of many ways a coalition can do this is by recognizing that they add value and warrant remuneration. Further, inviting the Community Champions to take a decisive role at the table reinforces the intrinsic value that they possess. Coalitions can engage those who might not otherwise have a voice and develop avenues for respectful dialogue and listening between diverse groups of stakeholders.
Vital Village Network
Vital Village Network is a network of residents and organizations in Boston committed to maximizing child, family, and community well-being. We mobilize collective investment from residents and community institutions to seed scalable and sustainable community change to promote healthy social and emotional development in early childhood. Vital Village utilizes a collective impact approach to enhance existing resources and align existing efforts focused on prenatal opportunity, early childhood education, and peer-to-peer advocacy. Our organization’s focus for the SCALE initiative has been the expansion and enhancement of the Peer-Advocate Action Roundtable (PAR) and Infusing Trauma-Informed Practices into Classrooms. The PAR project is a collaboration between the Medical-Legal Partnership and the Boston and Dudley Street Neighborhood Initiative that provides legal advocacy training to support peer-to-peer community lawyering efforts. Infusing Trauma-Informed Practices into Classrooms is a collaboration between the Child Witness to Violence Project and Vital Village Network and provides resources to students, teachers, and school administrators to improve emotional support for students, classroom organization strategies, and instructional support. To help facilitate the effectiveness, efficiency, and equity-focus of these projects (especially as they related to scalability and sustainability), we have been committed to embedding quality improvement methods (Langley et al., 2009) into all network activities.
Collaboration and Coalition Development
Initially, a need for cross-sector collaboration between partner organizations that utilize existing community resources inspired the formation of Vital Village Network. Many community-based organizations in the surrounding neighborhoods spend months designing and attempting to implement programs that are already being offered by other organizations. These efforts are often time and cost-intensive and tend to have a poor reach since similar programs already exist. Furthermore, many of these programs lack depth and breadth because they are focused on a specific need and may not address holistic well-being. The Vital Village Network is committed to reducing these occurrences through aligning existing efforts and spurring innovation where needed. Both SCALE projects are innovation pilots designed to grow into sustainable collaborative efforts. These collaborations have resulted in child development trainings for informal caregivers, the opening of a community garden, the formation of a drop-in breastfeeding group, and the development of a curriculum for trauma-informed group child care.
Community Inclusion and Partnership and Community Leadership and Mentoring
Vital Village Network is fundamentally committed to amplifying the community voice by partnering with organizations that deeply identify with this mission. The SCALE Community Champion also serves as the President of the Vital Village Community Partnership (VVCP), a group of resident leaders aiming to build neighborhood investment in child, family, and community well-being. VVCP has created numerous leadership opportunities for individuals whose skills and assets are often overlooked and underutilized. For example, one individual participating in PAR applied this knowledge to secure a public safety officer for her child’s school.
Community Education, Information, Dissemination, and Building Public Awareness and Program Evaluation
An integral component of promoting healthy social and emotional development in early childhood is determining what indicators to track and how to measure them. A public, accessible data dashboard is currently being developed that will involve three Community Champions. The champions will determine which indicators to include in the dashboard and how to disseminate this information within the community. Specifically, Community Champions will be responsible for 1) sharing findings from the data dashboard with community members; 2) obtaining feedback on how to modify and refine to specific indicators; 3) formulating action plans to address adverse outcomes; and 4) acknowledging and celebrating neighborhood resilience.
Program Evaluation is essential to the successful implementation and management of the Infusing Trauma-Informed Practices into Classrooms initiative. Staff members conduct classroom observations pre- and post-intervention and collect and analyze quantitative and qualitative data to measure improvements in classroom management. Recognizing that formative evaluation can help improve service delivery, staff engagement, meeting/event effectiveness, and other organizational processes, we have begun to use our data in a more dynamic and collaborative manner. This helped Vital Village develop several resources to enhance programming for our network partners, including tools to capture parent engagement at a family fun day, an interview to enhance a peer-led program, and evaluation forms for a community event.
These examples illustrate how community psychology competencies are deeply embedded in the structure and process of Vital Village Network and have been pivotal to its success.
San Gabriel Valley Healthy Cities Collaborative
San Gabriel Valley Healthy Cities Collaborative (SGVHCC) is a community coalition that includes four multi-sector partners in the San Gabriel Valley (SGV) of Southern California. SGV is a region with various small to midsize cities close to the dense metropolitan city of Los Angeles, and officially a part of the sprawling Los Angeles County. The region is home to approximately 1.5 million residents, living in a richly diverse and multicultural environment with a large immigrant population, primarily from Asian and Latin American countries. The four coalition organizations include a comprehensive cancer center, school district, and a city parks and recreation department (all three in the same city), along with a small grassroots community-based organization located in a different city 20 miles away. The ethnic composition of the neighborhood where the cancer center, school district, and city parks and recreation are located is predominantly Latino, while the neighborhood ethnic composition of the community-based organization is predominantly Latino and African American, but with an increasingly White, middle class population due to gentrification. The population in these neighborhoods is categorized largely as low-income, with high rates of obesity, low rates of exercising and healthy eating (greatly influenced by the lack of quality healthy foods within the neighborhoods).
The coalition’s approach to promoting community health is parallel to that of SCALE, which is in large part capacity building. As we strengthen our abilities to promote health with the support of the SCALE initiative, we seek to increase the capacity of youth in our communities so they can be fully engaged in promoting health. Our aim is to improve healthier living (as defined by healthier eating and exercising) in our under-resourced communities. The process of collaborating as a coalition toward achieving our aim has provided an opportunity to reflect on core competencies from community psychology that are fundamental for community engagement, including empowerment, community inclusion and partnership, community leadership and mentoring, and an ecological perspective.
Empowerment, Community Inclusion and Partnership, and Community Leadership and Mentoring
The three competencies of empowerment, community inclusion and partnership, and community leadership and mentoring, undergird a broader theme of engaging the community as equal partners by creating the environment for not only including their voices, but also developing their talents. The community we are engaging with includes ourselves within our coalition and high school youth living within our neighborhoods. Our hope is that the youth will be key in spreading knowledge, motivation, and new norms of healthier behavior through peer-to-peer education and advocacy in their neighborhoods. For the youth to develop into leaders in health promotion, an empowerment process and the right environment are essential. To accomplish this, there is a need for both integrating valuable knowledge and skills from researchers and the activism of the community. This involves synthesizing theory, systematic methodology, metrics, program evaluation skills, and a need for deeply engaging with the lived experiences of people in the community who are outside the “culture of research”.
Within our current coalition, we have been challenged to work together and promote health in two different cities/neighborhoods within the same county and geographic region but 20 miles apart. The community-based organization, located in a different city, joined the rest of the coalition organizations who have had an ongoing relationship for the past five years. During the union, there was a natural excitement for the new collaboration and genuine motivation to “join forces” for mutual benefit. However, in that process there was also a rush for implementing a youth peer-to-peer education program with the grassroots organization that had been created and implemented by the three organizations for the past five years.
There was a good intention to adapt the program to the new context and the input of youth in that context was obtained in doing so. The program, a health curriculum to develop the knowledge, skills, and leadership of youth to become community health educators, has shown initial promise. The program is being further developed in the setting where it has been implemented for the past five years. Additionally, we are engaging youth in this setting in a PhotoVoice project where we are seeing youth become empowered as they meet with and influence local policy makers about the needs and resources of their community toward health promotion and advocacy.
Ecological Perspective
The grassroots organization that is a part of our coalition and is located in a different city has been engaging youth in their setting on a project to create a “healthy living hub” that includes education and supports for healthier living. The vision of this project is to change the environment in the local neighborhood to improve access to healthy foods for all youth and their families. The rapid gentrification currently happening in this neighborhood and continuing disparities in resources, income, and other factors, points to the entrenched inequities and racism prevalent in our systems. The challenges faced by the grassroots organization tied to gentrification and local racial disparities challenged the other coalition partners to respect the need of this grassroots organization for other projects better tailored to their specific local neighborhood.
The different health projects in our two different cities reminds us of the distinction between a focus at the individual-level and system-level, as well as the challenges in changing behaviors through first vs. second-order change. The vision does not differ with respect to what the outcome should be - better health for our youth and communities - but the process of how to get there, due to contextual differences, is envisioned differently. Therefore, using the community psychology competency of an ecological perspective helps us to be sensitive to context and respecting the local social ecology and vision. In both contexts, there is the acknowledgement that the tools of research and activism/advocacy are helpful. Among our coalition, members may differ in placing an emphasis on research or community organizing or on what should be the particular project or method by which to achieve our aim. However, it is clear for all of us that promoting health equity is necessary and are becoming more keenly aware by applying an ecological perspective that the dynamic in a particular context will determine how the core competencies of empowerment, community inclusion and partnership, and community leadership and mentoring, along with others, are put into practice.
SCALE Formative Evaluation
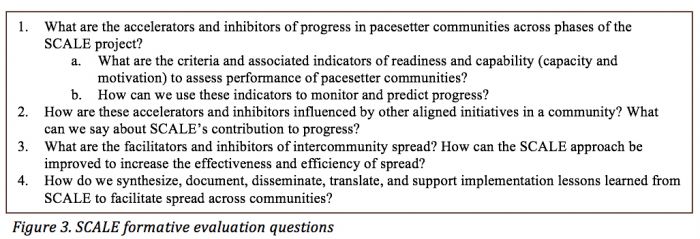
Community psychology competencies greatly inform how progress is evaluated in SCALE. We are using a formative evaluation approach to monitor ongoing program implementation and to provide guidance for improvement of SCALE supports. The evaluation team includes community psychologists and improvement scientists from the University of South Carolina, the University of North Carolina, and IHI. We are utilizing a collaborative approach to evaluation where we partner with the RWJF, the implementation team (IHI and community partners), and SCALE communities in the co-design of the evaluation plan and in the co-creation and synthesis of evaluation findings and use. The evaluation plan is driven by four broad questions (Figure 3). In this section, we describe how community psychology competencies promote meaningful collaboration and evaluation development, implementation and use that are grounded in empowerment and equity.
Figure 3. SCALE formative evaluation questions (See PDF version or JPG at the end of this article)
Ecological Perspective
Our work embraces an ecological perspective that captures implementation at multiple levels of analysis: 1) the implementation team level, specifically those activities implemented by the SCALE implementation team and community partners to all SCALE community coalitions (like training and tools), 2) intercommunity interactions and spread occurring between community coalitions, and 3) activities delivered locally within each community. Our ecological approach emphasizes understanding of how communities interact with the SCALE support system, how they engage with one another, and how change occurs in local contexts. This perspective ensures that feedback provided through the evaluation for program improvement is shared across systems and that evaluation methods are tailored and adapted to meet the needs of diverse stakeholders.
Sociocultural and Cross-cultural competence and Community Inclusion and Partnerships
Our evaluation approach also emphasizes sociocultural and cross-cultural competence and community inclusion and partnerships. We collaborate with SCALE communities to develop and review evaluation methods with the goal of enhancing their clarity and cultural relevance. For example, we share and pilot surveys with community representatives prior to implementation and revise per feedback. All evaluation results are shared with communities. Further, we communicate to communities how their feedback is used to inform program improvements. As an example, we used an approach called ‘you said, we did’ to share with communities how findings generated through their feedback were integrated to make requested changes to the program design.
Participatory Community Research
It is important to reflect on the effectiveness, efficiency and other quality indicators of the evaluation method and results. As part of our evaluation methods, we ask for feedback from the IHI implementation team and SCALE communities with the goal of assessing the quality of the evaluation itself. We ask questions regarding their perceived value of the evaluation approach and relevance, clarity and utility of evaluation methods and findings. Results from our first implementation of this method revealed a number of things, including that communities wanted to better understand our evaluation approach. Thus, we created a 1-page overview of our evaluation plan that was intended to communicate evaluation methods in an easy to understand format. Findings from this “evaluation of the evaluation,” also revealed that some communities found surveys burdensome. In response, we are actively working to revise our surveys to reduce the number of items and continue to explore further ways to reduce evaluation burden through alternative methods. We also heard that the IHI implementation team felt that our evaluation reports appeared to focus more on negative feedback from communities and we have thus revised our reports to include a broader range of responses.
Conclusion
In community health improvement work, community psychologists practically contribute in several ways that concretely align with the community psychology competencies. When reflecting upon each of our four settings, we collectively decided not to pre-specify what competencies we would discuss. Rather, we wanted each of us to share which competencies we believed were most salient in our work.
After reviewing our work, we found that there are extensive activities in which the community psychology competencies are applied. In particular, we note that the competency of community inclusion and partnership emerged as particularly relevant in our settings. Recognizing how power and privilege can separate stakeholders has proved instrumental in developing community health improvement projects that have tangible resonance for the community. Community inclusion (i.e., incorporating people with lived experience) is a particular driver in how SCALE hopes to foster health equity.
Furthermore, SCALE’s theory of change on how to increase health equity in communities directly parallels the community psychology competencies. Nearly all of the competencies can be practiced with an equity lens (e.g. collaboration development can be informed by developing relationships with organizations that have reach and representation with underserved communities.) SCALE’s framework for building communities’ abundance (Leading from Within, Leading Together, Leading for Outcomes, and Leading for Equity) can be concretely operationalized using the skills that community psychologists possess (Table 1). Each of the case examples describe the unique local and social determinants of health that impact low income communities of color and solutions to promote equity. The SCALE approach to abundance provides a guide for the processes and actions needed for equitable solutions.
We also recognize the importance of collective learning (evaluation and participatory research) as a method to promote action toward health equity. Apart from the examples in the SCALE formative evaluation, both San Gabriel and the Vital Village used evaluation methods as a tool to promote engagement among community members and to focus health equity work. Other specific examples of how the competencies can be used to address equity can be found in Vital Village collaboration structure, the capacity-building work of San Gabriel, and the emphasis on empowerment and prevention and health promotion (all projects). Furthermore, although we only discussed a portion of the competencies in each of our project reviews, we note that nearly all of the competencies are currently being applied in SCALE across settings. We summarize other areas of our work as it applies to SCALE in Table 1.
Concurrently, there is a rich history of public health practice that closely aligns with our work. Similar to the work of Dalton and Wolfe (2012), the Public Health Foundation (2014) has identified eight core competencies of for the practice of public health. These competencies are: 1) Analytical/Assessment, 2) Policy Development/Program Planning, 3) Communication, 4) Cultural Competency, 5) Community Dimensions of Practice, 6) Public Health Sciences; 7) Financial Planning and Management, and 8) Leadership and Systems Thinking. Each of the domains is further subdivided into three tiers that represent career stages for public health professionals: front line staff/entry level, program management/supervisory level, senior management/executive level. The tier format is a helpful heuristic for comparing and contrasting roles and responsibilities at various career stages, and something that would be useful to consider as the competencies of community psychology are applied to community health improvement. This type of structure may also help to facilitate additional training design for the next generation of community psychologist.
Although the core competencies of public health seem to broadly mirror community psychology, some critical distinctions exist. For example, instead of confining Community Dimensions of Practice Skills to one domain, these skills are embedded in all 18 community psychology competencies. Similarly, the Financial Planning and Management Skills domain includes a competency on addressing community health needs but does not explicitly mention engaging the community in this process. Community psychologists are charged with prioritizing the needs of the community regardless of their role, responsibilities, or work environment. Our experiences working in these case settings we described earlier, especially when trying to foster health equity, has reinforced this point. Furthermore, depending on their work environment, public health professionals may not be expected to master these competencies. Additionally, most public health programs are organized into specific analytical concentrations such as health policy and management, epidemiology, and biostatistics. Students focus their coursework on these topics, whereas community psychology training, in comparison, more heavily prioritizes relational skills to engage and empower their community throughout all activities. For these reasons, community psychologists may be well equipped to engage in collaborative community health improvement initiatives in public health professionals due to both the overlap and distinction between their practice skills. There is great potential for synergy through the use of these collective assets.
Based on our experiences and reflections, we believe that community health improvement is an appropriate setting for community psychologists to use a wide range of their competencies and skills to collaboratively work toward health improvement goals, especially when these goals include a focus on increasing health equity in communities. In this article, we have described how community psychologists have been able to apply their skills in community-based, collaborative projects designed to improve health and wellness in communities. Community psychologists who wish to work in these settings may find extensive and varied opportunities to use their skill set.
References
Agency for Healthcare Research and Quality. (2014). National Healthcare Disparities Report 2012. U.S. Department of Health and Human Services. Rockville, MD.
Association of State and Territorial Health Officials (2013). Role of the State and Territorial Health Official in Promoting Health Equity. Retrieved from. http://www.astho.org/Programs/Health-Equity/Health-Equity-Orientation-for-SHOs/
Campbell, C., & Murray, M. (2004). Community health psychology: Promoting analysis and action for social change. Journal of Health Psychology, 9(2), 187-195.
Dalton, J., & Wolfe, T. (2012) Competencies for Community Psychology Practice. The Community Psychologist, 45(4), 7-14.
Green L. W. (2008). Public health asks of community psychology… American Journal of Community Psychology, 41. 404-406.
Healthy People 2020 (May 26, 2016). Approach to the Social Determinants of Health. Retrieved from https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health
Institute for Healthcare Improvement. (2016). 100 Million Healthier Lives. Creating a Community of Solutions through a Culture of Abundance. Retrieved from http://www.ihi.org/Engage/Initiatives/100MillionHealthierLives/Documents/100%20Million%20Healthier%20Lives%20Brochure.pdf
Kania, J., & Kramer, M. (2011). Collective Impact. Stanford Social Innovation Review. Retrieved from: http://ssir.org/articles/entry/collective_impact.
Kania, J., & Kramer, M. (2013). Embracing Emergence: How Collective Impact Addresses Complexity. Stanford Social Innovation Review. Retrieved from: http://ssir.org/pdf/Embracing_Emergence_PDF.pdf
Kloos, B., Hill, J., Thomas, E., Wandersman, A., & Elias, M. (2011). Community psychology: Linking individuals and communities. Cengage Learning.
Kubota, J. T., Li, J., Bar-David, E., Banaji, M. R., & Phelps, E. A. (2013). The price of racial bias intergroup negotiations in the Ultimatum Game. Psychological Science, 24(12), 2498-2504.
Langley, G. J., Moen, R., Nolan, K. M., Nolan, T. W., Norman, C. L., & Provost, L. P. (2009). The improvement guide: a practical approach to enhancing organizational performance. John Wiley & Sons.
Mockenhaupt R. & Woodrum A. (2015). Developing evidence for structural approaches to build a culture of health: A perspective from the Robert Wood Johnson Foundation. Health Education and Behavior, 42 (IS): 152-19S.
Nelson, J., Spokane, L., Ross, L., & Deng, N. (2015). Advancing Racial Equity and Transforming Government. A Resources Guide to Put Ideas into Action. Government Alliance on Race & Equity. Retrieved from: http://racialequityalliance.org/newsite/wp-content/uploads/2015/02/GARE-Resource_Guide.pdf.
Public Health Foundation. (June 2014) Core Competencies for Public Health Professional. Retrieved from: http://www.phf.org/resourcestools/Documents/Core_Competencies_for_Public_Health_Professionals_2014June.pdf.
Society for Community Research and Action (2016). Who we are. Retrieved from. http://www.scra27.org/who-we-are/.
US Office of Minority Health. (2015). National stakeholder strategy for achieving health equity. US Department of Health and Human Services. Retrieved from. http://www.minorityhealth.hhs.gov/assets/pdf/FINAL_HHS_Action_Plan_Progress_Report_11_2_2015.pdf.
Wallerstein, N. B., & Duran, B. (2006). Using community-based participatory research to address health disparities. Health Promotion Practice, 7(3), 312-323.
Wallerstein, N., & Duran, B. (2010). Community-based participatory research contributions to intervention research: the intersection of science and practice to improve health equity. American journal of public health, 100(S1), S40-S4
Wolff, T. (2016). Ten Places Where Collective Impact Gets It Wrong. Global Journal of Community Psychology Practice. 7(1).
Download PDF version for full article including all tables, figures, and appendices.
 Jonathan P. Scaccia, Noé Rubén Chávez, Lena Hatchett, Kymberly Byrd, Shanika Blanton, Kassandra Alia, Laura Jean Brennan, Paul Howard, Niñon Lewis, Somava Stout
Jonathan P. Scaccia, Noé Rubén Chávez, Lena Hatchett, Kymberly Byrd, Shanika Blanton, Kassandra Alia, Laura Jean Brennan, Paul Howard, Niñon Lewis, Somava Stout
Jonathan P. Scaccia, PhD, is a practicing community psychologist who has extensive experience helping organizations select, adapt, implement, and evaluate improvement interventions. His current research focuses primarily on how readiness influences outcomes. This includes developing comprehensive methods to evaluate quantitative and qualitative differences in organizational readiness and enhancing strategies that can help to build readiness. Dr. Scaccia also works toward developing practical implementation science techniques that are usable by front-line practitioners, and facilitating the use of evidence-based implementation support strategies (e.g. technical assistance, quality improvement, etc.). Dr. Scaccia has his PhD in Clinical-Community Psychology from the University of South Carolina, and has previously completed a research fellowship in the Office of the Assistant Secretary for Health at the U.S. Department of Health and Human Services (OASH/HHS). Correspondence to this article should be addressed to Jonathan Scaccia, 1014 Hartman Road, Reading, PA, 19606: email. Jonathan.p.scaccia@gmail.com
Noé Rubén Chávez, PhD, is a postdoctoral research fellow in the Population Sciences department at the Beckman Research Institute, within the comprehensive cancer center of City of Hope, in Duarte, CA. He is a trained community psychologist with interests in youth empowerment, cultural competency, health equity, and community-based participatory research. One of his current projects involves working with an interdisciplinary team of scientists, including biologists and breast cancer researchers and clinicians, on developing, implementing, and evaluating programs to mentor and inspire children and adolescents of color to pursue science and health careers. As a community psychologist, his role is to assure that the science and health mentoring programs are developed, implemented and evaluated by working with local communities, engaging youth in participatory research, challenging traditional paradigms of science, and empowering youth of color to become leaders in achieving health equity.
Lena Hatchett, PhD, is a Social and Health Psychologist at Loyola University Chicago Neiswanger Institute for Bioethics. Her research focuses on community-based participatory action to promote health equity. Dr. Hatchett’s collaborative work in the area of local food justice founded the Maywood Multicultural Farmers Market and the Cook County Green Corps, a youth green job program. On-going projects include Proviso Partners for Health, a multi-sector coalition for community health and economic growth using policy, system, and environmental change strategies. You can read more about her work at Provisopartners.com. Beyond the local level, Dr. Hatchett is a member of the leadership team and the Health Equity hub for “100 Million Healthier Lives”, a multisector campaign to promote health, wellbeing and equity. This work is funded by RWJ foundation to the Institute for Healthcare Improvement for the SCALE initiative and the Trinity Health System Transforming Communities Initiative.
Kymberly Byrd, MSW, MPH, serves as the Project Manager for Vital Village Network at Boston Medical Center, a network of residents and organizations committed to maximizing child, family, and community well-being. She obtained her Bachelor's in Social Work and Spanish at Oakwood University in Huntsville, Alabama and her Master's in Social Work and Public Health at Boston University. She has research and evaluation experience in the fields of community engagement, homelessness, mental health, substance abuse, sexual health, HIV/AIDS, and maternal and child health. Personally and professionally, Kymberly is passionate about raising awareness about social justice issues and empowering people to take action.
Shanika Blanton, PhD is the Program Manager for Proviso Partners For Health (PP4H) in West Suburban Cook County, Illinois. Dr. Blanton’s role is to work with community and organizational partners through strategic planning and development, as well as program implementation and evaluation of specific aims addressing health equity and promoting the development of a green economy. Dr. Blanton also lectures at Loyola University Chicago in the Stritch School of Medicine in the Neiswanger Institute for Bioethics. As a community psychologist, Dr. Blanton is guided by a deep conviction that interdisciplinary and multi-faceted approaches that are co-lead and collaboratively designed with stakeholders from the communities they serve effect the most engaging and sustainable positive changes.
Kassandra Alia, MA, works as a member of the formative evaluation team for the Insitute for Healthcare Improvement's SCALE (Supporting Community Accelerators through Learning and Evaluation) initiative. Kassy is particularly passionate about addressing inequities in resources needed to live healthy lives and in working with organizations to use research and evaluation to build readiness for facilitating systems change efforts. She is currently working on her Ph.D. in Clinical-Community Psychology while working as an evaluator/consultant with a focus on the use of implementation support strategies for promoting community health.
Laura Brennan, MSW, has supported communities throughout the United States to create community-based coordinated systems of care that ensure better health for all people at less cost. Currently, Laura is the Co-Chair of the 100 Million Healthier Lives Leadership Team. Further, Laura is the Director of Pathway to Pacesetter, a 100 Million Healthier Lives program, supporting communities across the United States accelerate their efforts to promote health, well-being and equity. Previously, Laura supported rural Oregon communities to innovate and transform their systems of care while serving as the Community Affairs Senior Manager at CareOregon, a non-profit health plan that serves people enrolled in Medicaid and Medicare. Laura also worked for PacificSource Health Plans as their Community Development and Policy Director as well as the Executive Director of their Charitable Foundation. In addition, Laura worked for the State of Oregon in a variety of public policy and community health and development positions.
Paul Howard, MPA, is the Senior Director of Knowledge Sharing (KnoSh) at Community Solutions, leading their domestic and international consulting work. KnoSh uses its Agile Problem Solving methodology to improve systems and solve complex issues, particularly in the areas of homelessness, poverty alleviation and health. His work has included managing the launch of the Institute of Global Homelessness, the planning and launching of a 20,000 Homes Campaign in Canada and the European Campaign to End Street Homelessness and leading Community Solution’s efforts as a partner in 100 Million Healthier Live. Previously, Paul served as the Director of Data and Performance Management for Community Solution’s 100,000 Homes Campaign. Paul brings 20 years of experience working in human services, including direct services, system design, training, facilitation, performance management and consulting. Paul Holds a Masters in Public Administration from City University of New York, Baruch School of Public Affairs.
Niñon Lewis, MS, currently leads IHI’s Triple Aim for Populations Focus Area, which encompasses innovation, content, and programming in the areas of the Triple Aim, population health, population management, primary care, and community-wide improvement efforts. Over her time at IHI, her work has focused on leading large-scale initiatives on population health and the Triple Aim, including the IHI Triple Aim Improvement Community and the Scotland Early Years Collaborative. In addition, she has led IHI’s New Business Development team, developing large-scale programs and initiatives for the organization.
Somava Stout, MD, MS is the Executive Lead of 100 Million Healthier Lives, a global partnership initiative convened by the Institute for Healthcare Improvement (IHI) that aims to support thousands of people, organizations and communities to develop the capacity to achieve breakthrough improvements in health, wellbeing and equity. She is the Principal Innovator for SCALE, which helps 24 communities in the US to become communities of solution. She has worked with health systems and communities across the globe to achieve sustainable large-scale transformation in health and human development for over 20 years. Previously, as a Vice President at Cambridge Health Alliance, she led a large-scale transformation of a Harvard safety net system from volume to value that achieved breakthrough results and earned numerous national accolades, including the Robert Wood Johnson Foundation Young Leader Award in 2012 for her contributions to the health and healthcare of the nation. She also served as the Co-Director of Leadership Programs at the Harvard Medical School Center for Primary Care, where she developed faculty and student leaders in innovation, improvement and implementation.
Add Comment
![]() Download the PDF version to access the complete article.
Download the PDF version to access the complete article.
Keywords: Community health improvement, coalitions, SCALE, health equity, socio-cultural competence, diverse contexts
 Based on a work at www.gjcpp.org.
Based on a work at www.gjcpp.org.